Open Journal of Obstetrics and Gynecology
Vol.06 No.03(2016), Article ID:64088,10 pages
10.4236/ojog.2016.63020
The Effect of Insulin Resistance on In-Vitro Fertilization-Embryo Transfer in Women without Polycystic Ovary Syndrome
Keiko Mekaru*, Sugiko Oishi, Kozue Akamine, Tadatsugu Kinjo, Chiaki Heshiki, Hitoshi Masamoto, Yoichi Aoki
Department of Obstetrics and Gynecology, Graduate School of Medicine, University of the Ryukyus, Nishihara, Okinawa, Japan

Copyright © 2016 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution-NonCommercial International License (CC BY-NC).
http://creativecommons.org/licenses/by-nc/4.0/



Received 31 October 2015; accepted 27 February 2016; published 1 March 2016
ABSTRACT
Purpose: Insulin resistance (IR) plays an important role in the pathogenesis of polycystic ovary syndrome (PCOS); therefore, insulin-sensitizing agents are widely used to improve IR in women with PCOS. However, whether IR in patients without PCOS should be treated remains uncertain. This study aims to clarify whether IR in patients without PCOS affects the outcomes of in-vitro fertilization-embryo transfer (IVF-ET) and pregnancy. Methods: Between January 2011 and December 2013, we retrospectively reviewed the medical records of 116 non-PCOS patients who underwent the first IVF?ET cycle. IR was calculated using the homeostasis model assessment (HOMA) index [HOMA-IR = (insulin × glucose)/405]. A HOMA index of >2.5 was used to indicate IR. Based on the HOMA index calculation, 28 patients were IR(+) and 88 patients had normal insulin sensitivity. We retrospectively compared the response with controlled ovarian hyperstimulation, retrieved oocytes number, fertilization rates, pregnancy rate, live birth rates, and gestational diabetes mellitus (GDM) incidence. Results: There were no significant differences in human menopausal gonadotropin administration, peak estradiol, retrieved oocyte number, fertilized embryo number, good quality embryo number, implantation rate, clinical pregnancy rate, miscarriage rate, delivery rate, or ovarian hyperstimulation syndrome and GDM incidences between the groups. Conclusion: IR in non-PCOS patients has no effect on IVF-ET outcomes or perinatal prognosis.
Keywords:
Insulin Resistance, Polycystic Ovary Syndrome, In-Vitro Fertilization-Embryo Transfer, Gestational Diabetes Mellitus

1. Introduction
Insulin levels have been suggested to play important roles in fertility and folliculogenesis within the setting of assisted reproductive technology (ART). Insulin primarily acts on its own receptors located on theca cells, which surround stroma and granulosa cells, to stimulate ovarian steroidogenesis [1] - [3] . In the context of polycystic ovary syndrome (PCOS), hyperinsulinemia, resulting from increased insulin resistance (IR), is associated with a higher rate of ovulatory infertility [4] . Conversely, in response to gonadotropin stimulation for in vitro fertilization (IVF), IR is frequently associated with a multifollicular response; thus, patients with IR are more prone to ovarian hyperstimulation syndrome (OHSS) and ART cycle cancelation [5] [6] . In addition, women with PCOS have poorer oocyte quality, resulting in lower fertilization and cleavage rates, than normal women [7] - [10] . Hyperinsulinemia can preferentially impair oocyte developmental competence, resulting in reduced fertilization rates, embryonic development, and implantation in PCOS patients [11] - [13] . The administration of insulin-sen- sitizing agents increases insulin sensitivity, thereby promoting ovulation induction and increasing the pregnancy rate [14] [15] . Metformin is the most studied antidiabetic drug and is administered to reduce fasting insulin, luteinizing hormone (LH), and free testosterone levels in an effort to restore menstrual cyclicity and fertility [16] . We hypothesized that numerous oocytes of lower quality could be harvested from non-PCOS patients with IR, identical to the observations in PCOS patients. If this hypothesis is true, insulin sensitization treatment could be included as a treatment option for non-PCOS patients with IR. Therefore, the aim of this study was to clarify whether IR in non-PCOS patients affects IVF and pregnancy outcomes.
2. Materials and Methods
2.1. Subjects
We retrospectively reviewed the patient records of 116 female non-PCOS patients who underwent first embryo transfer (ET) from January 2010 to December 2012. Inclusion criteria were a regular menstrual cycle and no sign of polycystic ovaries on ultrasound. Women diagnosed with PCOS were excluded. Diagnosis of PCOS was based on the 2007 guidelines of the Japan Society of Obstetrics and Gynecology: 1) amenorrhea or oligomenorrhea, 2) clinical or biochemical hyperandrogenism or high LH and normal follicle-stimulating hormone (FSH) levels, and 3) polycystic morphology on ultrasound (at least one ovary must contain 10 or more small cysts measuring 2 - 9 mm in diameter) [17] [18] . Women with endocrine disorders, including diabetes mellitus; hepatic and cardiovascular disorders; hyperandrogenemia, such as congenital adrenal hyperplasia, hyperprolactinemia, or androgen-secreting neoplasia; and other concurrent gynecological disorders were also excluded. The study protocol was approved by the ethical review board of the University of the Ryukyus (Okinawa, Japan), and all patients submitted written, informed consent before participation in this study.
2.2. Endocrine and Metabolic Assessment
Baseline hormone levels were measured in blood samples collected after overnight fasting on day 2 or 3 of the menstrual cycle prior to the commencement of an IVF-ET cycle.
Basal serum levels of FSH, LH, estradiol (E2), thyroid-stimulating hormone, and prolactin were determined using appropriate laboratory assays, including electrochemiluminescence assay and radioimmunoassay (all obtained from Roche Diagnostics Co., Ltd., Tokyo, Japan). Lipid profile, including total cholesterol (Kyowa Medex Co., Ltd., Tokyo, Japan), high-density lipoprotein cholesterol (Sekisui Medical Co., Ltd., Tokyo, Japan), low-density lipoprotein cholesterol (Sekisui Medical Co., Ltd., Tokyo, Japan), and triglycerides (TG; Kyowa Medex Co., Ltd., Tokyo, Japan), of each patient was assessed. Serum insulin was assayed using a competitive chemiluminescent enzyme immunoassay performed on the Lumipulse® Presto® II automated system (Fujirebio Co., Ltd., Tokyo, Japan). The analytical sensitivity of the insulin assay was 0.3 µIU/ml, the coefficient of variation was 10%, and there was no stated cross-reactivity with proinsulin. Plasma glucose levels were measured using the Quickauto NEO reagent (Shinotesuto Co., Ltd., Kanagawa, Japan). IR was calculated by the homeostasis model assessment (HOMA) index [HOMA-IR = (insulin × glucose)/405]. A HOMA index of >2.5 indicated the presence of IR [19] . HOMA index is a validated surrogate marker for IR and has a good agreement with the gold standard hyperinsulinemic euglycemic clamp test [20] .
2.3. IVF-ET
Controlled ovarian stimulation was performed using the gonadotropin-releasing hormone agonist buserelin acetate (Suprecur®; Mochida Pharmaceutical Co., Ltd., Tokyo, Japan), which was intranasally administered at a dose of 900 μg/day from day 2 of the stimulation cycle to the day of human chorionic gonadotropin (hCG) injection (10,000 IU; Gonatropin, Asuka Pharmaceutical Co., Ltd., Tokyo, Japan). An initial dose of 300 IU/day of human menopausal gonadotropin (HMG; Teizo, Tokyo, Japan) was administered on day 3 of the cycle, followed by 225 IU/day of HMG. hCG was administered when the diameter of the two ovarian follicles were ≥18 mm. Peak E2 levels were measured before hCG administration. Transvaginal oocyte retrieval was performed 35 h after hCG administration. Oocytes were fertilized either by conventional IVF-ET or by intracytoplasmic sperm injection (ICSI) 4 h after retrieval. ICSI was performed for couples experiencing infertility due to a male factor. Embryos were cultured in early cleavage medium™ (IS Japan Co., Ltd., Saitama, Japan) in an atmosphere containing 5% CO2, 5% O2, and 89% N2 at 37˚C in an incubator (Astec Co., Ltd., Fukuoka, Japan). Embryo quality was evaluated on the basis of Veeck’s criteria, with high-quality embryos classified as grade 1. One or two embryos were transferred 3 days after oocyte retrieval using ET catheters (Kitasato Supply, Shizuoka, Japan) under ultrasound guidance. For luteal phase support, 5000 IU of hCG was injected on the day of oocyte retrieval and then on days 3 and 7. The World Health Organization classification was used for OHSS assessment. When seven or more oocytes were retrieved, surplus oocytes were cryopreserved to prevent OHSS. Day 3 cleaved embryos were vitrified by the Cryotop method on day 3, and after 2 months, the embryos were transferred. In the thawed ET cycle, transdermal E2 (Estrana®; Hisamitu Tokyo, Japan) was used in combination with an oral progesterone (P) suppository (Chlormadinone Acetate, FUJI Pharma, Toyama, Japan) for hormonal replacement. Preparation of the endometrium was started on day 2 of the hormonal replacement cycle and was achieved using a step-up regime (1.44 - 2.88 mg). The P suppository (12 mg/day) was started on day 15. Clinical pregnancy was defined by the presence of a gestational sac and fetal heartbeat. The main outcome measures were response to controlled ovarian hyperstimulation, retrieved oocyte number, clinical pregnancy rate, miscarriage rate, live birth rate, gestational diabetes mellitus (GDM) incidence, pregnancy-induced hypertension (PIH), premature delivery, and cesarean section.
2.4. Statistical Analysis
Proportions were compared using the Fisher’s exact test or chi-square test. Continuous variables were analyzed and compared using the Student’s t-test or Mann-Whitney U test. A probability (p) value of <0.05 was considered statistically significant. JMP software (SAS Institute, Inc., Cary, NC, USA) was used for the statistical analyses.
3. Results
Based on the HOMA index calculation, 28 patients had IR, whereas 88 patients had normal insulin sensitivity. Characteristics of both patient groups are shown in Table 1. Body mass index (BMI) tended to be higher in the IR group but not significantly. No significant differences in age, basal FSH and LH/FSH levels, and lipid profiles were observed between the groups. The HOMA index was significantly higher in the IR(+) group than in the IR(−) group (5 ± 2.8 vs. 0.2 ± 0.8, p < 0.001), whereas there was no significant difference in the glucose levels or causes of infertility between the groups.
Furthermore, there were no significant differences in HMG administration days (8.7 ± 2.2 vs. 8.9 ± 0.3, p = 0.46), peak E2 levels (2352.6 ± 1524 vs. 2373 ± 1850 pg/ml, p = 0.97), retrieved oocyte number (8.7 ± 6.5 vs. 8.9 ± 4.7, p = 0.55), fertilized embryo number (4.7 ± 3.6 vs. 4.3 ± 3.0, p = 0.34), high quality embryos (G1; % of all fertilized embryos, 23.4% vs. 15.2%, p = 0.48), or OHSS incidence (one case each) between the IR(+) and IR(−) groups (Table 2). To prevent OHSS, 12 (42.9%) and 24 (27.3%) patients in the IR(+) and IR(−) groups, respectively, underwent ET with thawed cryopreserved oocytes. There were no significant differences in implantation rate (39.3% vs. 29.5%, p = 0.29), clinical pregnancy rate (32.1% vs. 26.1%, p = 0.46), delivery rate (17.9% vs. 15.9%, p = 0.4), miscarriage rate (33.3% vs. 39.1%, p = 0.76), or incidences of GDM, PIH, prema-

Table 1. Characteristics of patients in the IR(+) and IR(−) groups.
*Values are expressed as mean ± standard deviation.
Table 2. IVF-ET outcomes in the IR(+) and IR(−) groups.
*Values are expressed as mean ± standard deviation.
ture delivery, and cesarean section between the two groups (Table 3). There was a significant correlation between the HOMA index and BMI (r2 = 0.2, p = 0.0001; Figure 1). Although we hypothesized that the HOMA index would increase with age, there was no such correlation (r2 = 0.07e−3, p = 0.9; Figure 2). There was a tendency to retrieve fewer oocytes as BMI increased (r2 = 0.05, p = 0.078; Figure 3). There was no correlation between the HOMA index and number of retrieved oocytes (r2 = 0.002, p = 0.71; Figure 4).
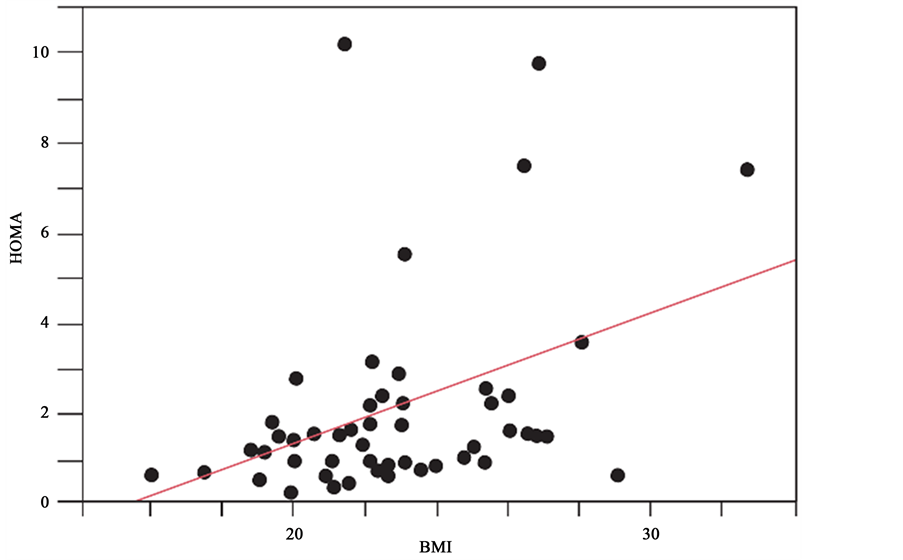
Figure 1. Correlation between the HOMA index and BMI. There was a significant correlation between the HOMA index and BMI (r2 = 0.2, p = 0.0001).
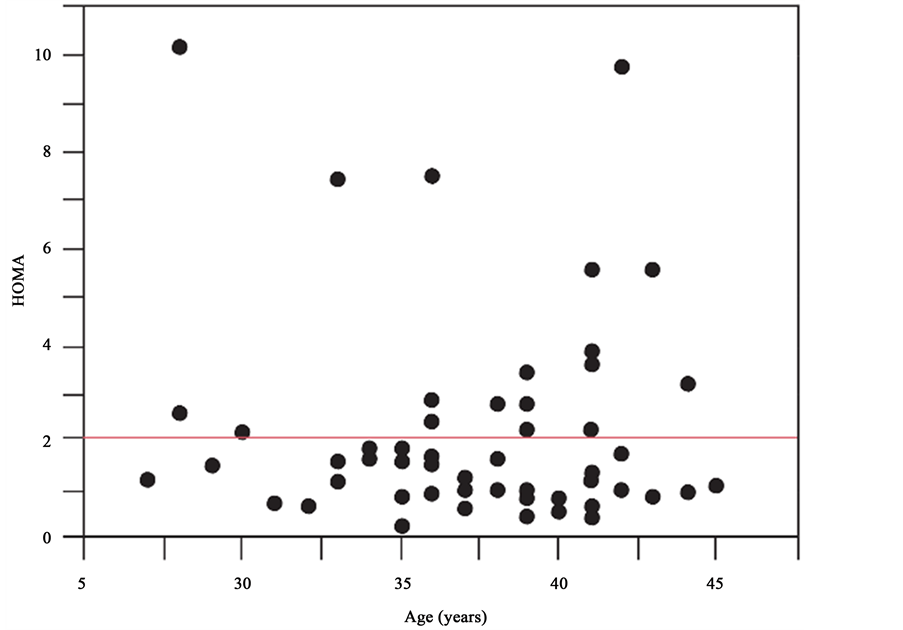
Figure 2. Correlation between the HOMA index and age. There was no correlation between the HOMA index and age (r2 = 0.07e−3, p = 0.9).
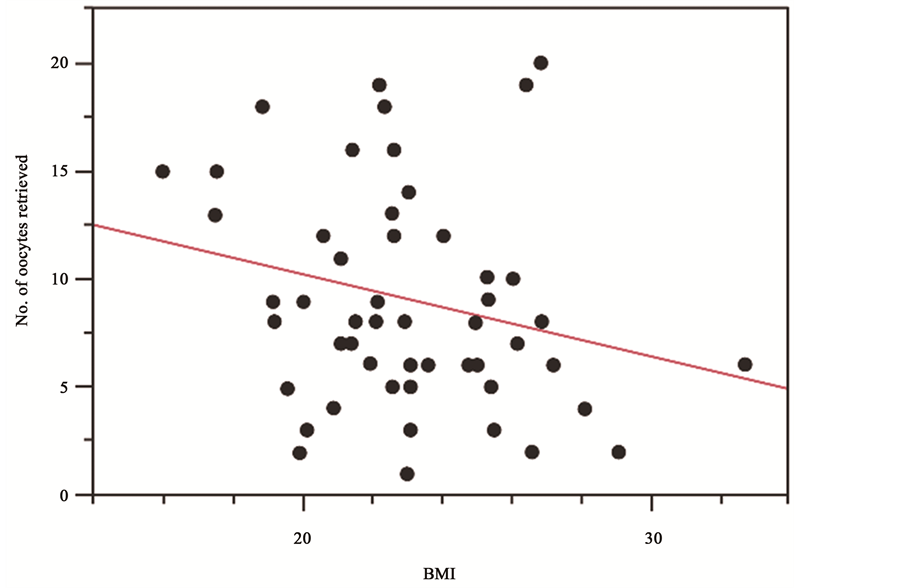
Figure 3. Correlation between BMI and number of oocytes retrieved. The number of retrieved oocytes tended to decrease with an increase in BMI (r2 = 0.05, p = 0.078).
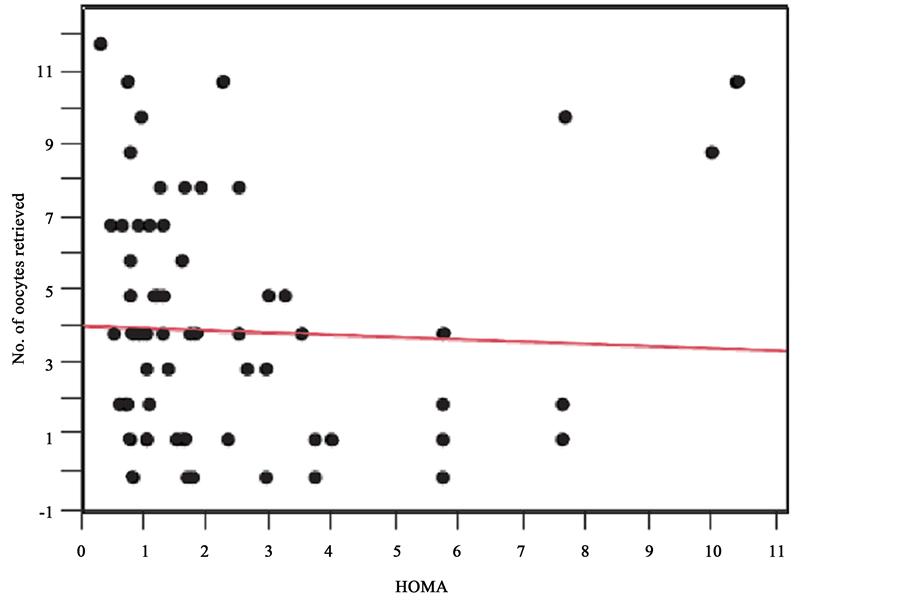
Figure 4. Correlation between the HOMA index and number of oocytes retrieved. There was no correlation between the HOMA index and retrieved oocytes number (r2 = 0.002, p = 0.71).
Table 3. Pregnancy outcomes in the IR(+) and IR(−) groups.
4. Discussion
The present study is the first to investigate pregnancy outcomes in non-PCOS patients with and without IR following IVF. We hypothesized that more oocytes could be retrieved from non-PCOS patients with IR, but of poorer quality, than from non-PCOS patients without IR. If this hypothesis was true, insulin sensitization treatment could be included as a treatment option for non-PCOS women with IR. However, the present study showed that IR did not significantly affect the required HMG dose, peak E2 level, retrieved oocyte number, fertilized egg number, OHSS incidence, embryo quality, fertilization rate, clinical pregnancy rate, or miscarriage rate.
Dickerson et al. investigated the impact of the HOMA index and androgen levels on IVF outcomes in 49 non-PCOS patients and found a significant correlation between the free androgen index and total follicle count in patients who underwent controlled ovarian hyperstimulation [21] . They also reported that nine patients with a HOMA-IR of ≥2.5 had significantly higher total follicle counts than 40 patients without IR. However, as in our study, they found no significant difference in the HMG dosage, retrieved oocyte number, or fertilized egg number.
In developing follicles, insulin receptors are expressed by granulosa and theca cells, and insulin is reported to cause primordial follicles to develop into primary follicles [22] . Furthermore, when follicles enter the gonadotropin-dependent stage, insulin growth factors amplify the response to FSH in granulosa cells [22] . Several studies have reported a correlation between hyperinsulinemia and IR in PCOS patients with oocyte maturation and ovulation [14] [23] . On the basis of these results, Dickerson et al. hypothesized that hyperinsulinemia was associated with an increase in the number of follicles [21] . However, they reported no significant difference in the number of retrieved oocytes between patients with and without IR.
Nafiye et al. compared the insulin levels in the serum and follicular fluid among nonobese patients with PCOS, patients with male infertility factors, and patients with unexplained infertility [24] . Although the nonobese PCOS patients had significantly higher serum insulin levels than the other two groups, there was no significant difference in intrafollicular insulin levels among the three groups. In addition, there was no correlation between the follicular fluid insulin levels and number of developing follicles in PCOS patients. These results suggest that a high serum insulin level does not necessarily result in a high follicular fluid insulin level and that there is no correlation between hyperinsulinemia and the number of developing follicles.
Nardo et al. reported a correlation between IR and elevated anti-Müllerian hormone in non-PCOS patients [25] . However, when the analysis was adjusted for age, there was no evident correlation. Thus, in a clinical setting, the presence of hyperinsulinemia may not influence the number of retrieved oocytes or frequency of OHSS. Fedorcsak et al. reported that obesity affects retrieved oocyte number and oocyte quality more than IR in PCOS patients [26] . In the present study, there was no correlation between IR level and retrieved oocyte number. Conversely, the number of retrieved oocytes tended to decrease as BMI increased (Figure 1).
For PCOS patients, although the number of retrieved oocytes increased following IVF, the oocyte quality, fertility rate, and implantation rate decreased and miscarriage rate increased [8] - [10] [27] [28] . In PCOS patients, various factors, including endocrine and local paracrine/autocrine actions, directly and indirectly interfere with oocyte maturation. The influence of extraovarian factors (i.e., LH hypersecretion, hyperandrogenemia, and hyperinsulinemia) and intraovarian factors (i.e., epidermal, fibroblast, insulin-like, and neurotrophin growth factors) is conceivable [29] . Many of these extraovarian and/or intraovarian factors may cause granulosa cell- oocyte interactions and oocyte maturation, which may potentially affect embryonic developmental competence. However, extraovarian and/or intraovarian factors may not play a role in non-PCOS patients. The findings of the present study suggest that only hyperinsulinemia does not promote an increase in retrieved oocyte number or decrease in oocyte quality, fertilization rate, or pregnancy rate.
In PCOS patients, the onset rate of GDM was significantly higher [30] -[32] , and the rates of pregnancy-in- duced hypertension, preeclampsia, premature delivery, and cesarean section were elevated [31] . Many infants had significantly lower birth weights and required treatment in a neonatal intensive care unit. However, in the present study, no significant difference in the frequency of GDM, premature delivery, or cesarean section was observed between patients with and without IR. Although only a few studies have investigated regarding this topic, we propose that IR is less likely associated with comparatively low pregnancy outcomes in non-PCOS patients.
5. Conclusion
In conclusion, despite the small number of participants in this study, the results suggest that IR in non-PCOS patients has no effect on IVF outcome or perinatal prognosis. However, a large-scale prospective study is necessary to clarify the effects of IR on pregnancy outcome.
Acknowledgements
The authors would like to thank Enago (www.enago.jp) for the English language review. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Cite this paper
KeikoMekaru,SugikoOishi,KozueAkamine,TadatsuguKinjo,ChiakiHeshiki,HitoshiMasamoto,YoichiAoki, (2016) The Effect of Insulin Resistance on In-Vitro Fertilization-Embryo Transfer in Women without Polycystic Ovary Syndrome. Open Journal of Obstetrics and Gynecology,06,157-166. doi: 10.4236/ojog.2016.63020
References
- 1. Samoto, T., Maruo, T., Ladines-llave, C., et al. (1993) Insulin Receptor Expression in the Follicular and Stroma Compartments of the Human Ovary over the Course of Follicular Growth, Regression, and Atresia. Endocrine Journal, 40, 715-726.
http://dx.doi.org/10.1507/endocrj.40.715 - 2. Franks, S., Gilling-Smith, C., Watson, H. and Willis, D. (1999) Insulin Action in the Normal and Polycystic Ovary. Endocrinology and Metabolism Clinics of North America, 28, 361-378.
http://dx.doi.org/10.1016/S0889-8529(05)70074-8 - 3. Kezele, P.R., Nilsson, E.E. and Skinner, M.K. (2002) Insulin But Not Insulin-Like Growth Factor-1 Promotes the Primordial to Primary Follicle Transition. Molecular and Cellular Endocrinology, 192, 37-43.
http://dx.doi.org/10.1016/S0889-8529(05)70074-8 - 4. Robinson, S., Kiddy, D., Gelding, S.V., et al. (1993) The Relationship of Insulin Sensitivity to Menstrual Pattern in Women with Hyperandrogenism and Polycystic Ovaries. Clinical Endocrinology, 39, 351-355.
http://dx.doi.org/10.1111/j.1365-2265.1993.tb02376.x - 5. Fulghesu, A.M., Villa, P., Pavone, V., et al. (1997) The Impact of Insulin Secretion on the Ovarian Response to Exogenous Gonadotropins in Polycystic Ovary Syndrome. The Journal of Clinical Endocrinology and Metabolism, 82, 644-648.
http://dx.doi.org/10.1210/jcem.82.2.3727 - 6. Dale, P.O., Tanbo, T., Haug, E. and Abyholm, T. (1998) The Impact of Insulin Resistance on the Outcome of Ovulation Induction with Low-Dose Follicle Stimulating Hormone in Women with Polycystic Ovary Syndrome. Human Reproduction, 13, 567-570.
http://dx.doi.org/10.1093/humrep/13.3.567 - 7. Sengoku, K., Tamate, K., Takuma, N., Yoshida, T., Goishi, K. and Ishikawa, M. (1997) The Chromosomal Normality of Unfertilized Oocytes from Patients with Polycysticovarian Syndrome. Human Reproduction, 12, 474-477.
http://dx.doi.org/10.1093/humrep/12.3.474 - 8. Mulders, A.G., Laven, J.S., Imani, B., Eijkemans, M.J. and Fauser, B.C. (2003) IVF Outcome in Anovulatory Infertility (WHO Group 2)—Including Polycystic Ovary Syndrome Following Previous Unsuccessful Ovulation Induction. Reproductive BioMedicine Online, 7, 50-58.
http://dx.doi.org/10.1016/S1472-6483(10)61728-2 - 9. Heijnen, E.M., Eijkemans, M.J., Hughes, E.G., Laven, J.S., Macklon, N.S. and Fauser, B.C. (2006) A Metaanalysis of Outcomes of Conventional IVF in Women with Polycystic Ovary Ssyndrome. Human Reproduction Update, 12, 13-21.
http://dx.doi.org/10.1093/humupd/dmi036 - 10. Sahu, B., Ozturk, O., Ranierri, M. and Serhal, P. (2008) Comparison of Oocyte Quality and Intracytoplasmic Sperm Injection Outcome in Women with Isolated Polycystic Ovaries or Polycystic Ovarian Syndrome. Archives of Gynecology and Obstetrics, 277, 239-244.
http://dx.doi.org/10.1007/s00404-007-0462-x - 11. Cano, F., Garcia-Velasco, J.A., Millet, A., Remohí, J., Simón, C. and Pellicer, A. (1997) Oocyte Quality in Polycystic Ovaries Revisited: Identification of a Particular Subgroup of Women. The Journal of Assisted Reproduction and Genetics, 14, 254-261.
http://dx.doi.org/10.1007/BF02765826 - 12. Jabara, S. and Coutifaris, C. (2003) In Vitro Fertilization in the PCOS Patient: Clinical Considerations. Seminars in Reproductive Medicine, 21, 317-324.
http://dx.doi.org/10.1055/s-2003-43310 - 13. Dumesic, D.A. and Abbott, D.H. (2008) Implications of Polycystic Ovary Syndrome on Oocyte Development. Seminars in Reproductive Medicine, 26, 53-61.
http://dx.doi.org/10.1055/s-2007-992925 - 14. Vandermolen, D.T., Ratts, V.S., Evans, W.S., Stovall, D.W., Kauma, S.W. and Nestler, J.E. (2001) Metformin Increases the Ovulatory Rate and Pregnancy Rate from Clomiphene Citrate in Patients with Polycystic Ovary Syndrome Who Are Resistant to Clomiphene Citrate Alone. Fertility and Sterility, 75, 310-315.
http://dx.doi.org/10.1016/S0015-0282(00)01675-7 - 15. Tang, T., Lord, J.M., Norman, R.J., Yasmin, E. and Balen, A.H. (2012) Insulin-Sensitising Drugs (Metformin, Rosiglitazone, Pioglitazone, D-chiro-inositol) for Women with Polycystic Ovary Syndrome, Oligo Amenorrhoea and Subfertility. The Cochrane Database of Systemic Reviews, No. 5, CD003053.
http://dx.doi.org/10.1002/14651858.CD003053.pub5 - 16. Krstevska, B., Dimitrovski, C., Pemovska, G., et al. (2006) Metformin Improves Menstrual Patterns, Endocrine and Metabolic Profile in Obese Hyperinsulinemic Women with a Polycystic Ovary Syndrome. Prilozi, 27, 57-66.
- 17. The Japanese Society of Obstetrics and Gynecology (2007) Constitute of Reproductive Endocrinology. Reports of a New Diagnostic Criteria of PCOS in Japan. Acta Obstetrica Et Gynaecologica Japonica, 59, 868-886.
- 18. Kubota, T. (2013) Update in Polycystic Ovary Syndrome: New Criteria of Diagnosis, and Treatment in Japan. Reproductive Medicine and Biology, 12, 71-77.
http://dx.doi.org/10.1007/s12522-013-0145-1 - 19. Matthews, D.R., Hosker, J.P., Rudenski, A.S., Naylor, B.A., Treacher, D.F. and Turner, R.C. (1985) Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia, 28, 412-419.
http://dx.doi.org/10.1007/BF00280883 - 20. Bonora, E., Targher, G., Alberiche, M., et al. (2000) Homeostasis Model Assessment Closely Mirrors the Glucose Clamp Technique in the Assessment of Insulin Sensitivity: Studies in Subjects with Various Degrees of Glucose Tolerance and Insulin Sensitivity. Diabetes Care, 23, 57-63.
http://dx.doi.org/10.2337/diacare.23.1.57 - 21. Dickerson, E.H., Cho, L.W., Maguiness, S.D., Killick, S.L., Robinson, J. and Atkin, S.L. (2010) Insulin Resistance and Free Androgen Index Correlate with the Outcome of Controlled Ovarian Hyperstimulation in Non-PCOS Women Undergoing IVF. Human Reproduction, 25, 504-509.
http://dx.doi.org/10.1093/humrep/dep393 - 22. Monget, P. and Bondy, C. (2000) Importance of the IGF System in Early Folliculogenesis. Molecular and Cellular Endocrinology, 163, 89-93.
http://dx.doi.org/10.1016/S0303-7207(99)00244-0 - 23. Nestler, J.E., Jakubowicz, D.J., Evans, W.S. and Pasquali, R. (1998) Effects of Metformin on Spontaneous and Clomiphene-Induced Ovulation in the Polycystic Ovary Syndrome. The New England Journal of Medicine, 338, 1876-1880.
http://dx.doi.org/10.1056/NEJM199806253382603 - 24. Nafiye, Y., Sevtap, K., Muammer, D., Emre, O., Senol, K. and Leyla, M. (2010) The Effect of Serum and Intrafollicular Insulin Resistance Parameters and Homocysteine Levels of Nonobese, Nonhyperandrogenemic Polycystic Ovary Syndrome Patients on in Vitro Fertilization Outcome. Fertility and Sterility, 93, 1864-1869.
http://dx.doi.org/10.1016/j.fertnstert.2008.12.024 - 25. Nardo, L.G., Yates, A.P., Roberts, S.A., Pemberton, P. and Laing, I. (2009) The Relationships between AMH, Androgens, Insulin Resistance and Basal Ovarian Follicular Status in Non-Obese Subfertile Women with and without Polycystic Ovary Syndrome. Human Reproduction, 24, 2917-2923.
http://dx.doi.org/10.1093/humrep/dep225 - 26. Fedorcsak, P., Dale, P.O., Storeng, R., Tanbo, T. and Abyholm, T. (2001) The Impact of Obesity and Insulin Resistance on the Outcome of IVF or ICSI in Women with Polycystic Ovarian Syndrome. Human Reproduction, 16, 1086-1091.
http://dx.doi.org/10.1093/humrep/16.6.1086 - 27. Ludwig, M., Finas, D.F., Al-Hasani, S., Diedrich, K. and Ortmann, O. (1999) Oocyte Quality and Treatment Outcome in Intracytoplasmic Sperm Injection Cycles of Polycystic Ovarian Syndrome Patients. Human Reproduction, 14, 354-358.
http://dx.doi.org/10.1093/humrep/14.2.354 - 28. Boomsma, C.M., Fauser, B.C.J.M. and Macklon, N.S. (2008) Pregnancy Complications in Women with Polyscystic Ovary Syndrome. Seminars in Reproductive Medicine, 26, 72-84.
http://dx.doi.org/10.1055/s-2007-992927 - 29. Qiao, J. and Feng, H.L. (2011) Extra- and Intra-Ovarian Factors in Polycystic Ovary Syndrome: Impact on Oocyte Maturation and Embryo Developmental Competence. Human Reproduction Update, 17, 17-33.
http://dx.doi.org/10.1093/humupd/dmq032 - 30. Boomsma, C.M., Eijkemans, M.J., Hughes, E.G., Visser, G.H., Fauser, B.C. and Macklon, N.S. (2006) A Meta-Analysis of Pregnancy Outcomes in Women with Polycystic Ovary Syndrome. Human Reproduction Update, 12, 673-683.
http://dx.doi.org/10.1093/humupd/dml036 - 31. Qin, J.Z., Pang, L.H., Li, M.J., Fan, X.J., Huang, R.D. and Chen, H.Y. (2013) Obstetric Complications in Women with Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. Reproductive Biology and Endocrinology, 11, 56.
http://dx.doi.org/10.1186/1477-7827-11-56 - 32. Wang, Y., Zhao, X., Zhao, H., et al. (2013) Risks for Gestational Diabetes Mellitus and Pregnancy-Induced Hypertension Are Increased in Polycystic Ovary Ssyndrome. Biomed Research International, 2013, Article ID: 182582.
NOTES

*Corresponding author.