Open Journal of Obstetrics and Gynecology
Vol.3 No.7B(2013), Article ID:36895,3 pages DOI:10.4236/ojog.2013.37A2002
Lost and found
![]()
1Department of Surgery, Bankstown Hospital, Sydney South West Area Health Service, Bankstown, Australia
2Faculty of Medicine, South Western Sydney Clinical School, University of New South Wales, Liverpool, Australia
Email: Dr.DeLacavalerie@gmail.com
Copyright © 2013 De Lacavalerie Penelope et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 3 June 2013; revised 5 July 2013; accepted 12 July 2013
Keywords: Laparoscopic Surgery; Intrauterine Device; Migration; Uterine Perforation
ABSTRACT
The insertion of intrauterine devices is a common procedure performed all over the world. In some circumstances, however, complications after this procedure can be latent.
1. INTRODUCTION
Intrauterine devices (IUDs) are commonly implanted as a contraceptive aid all over the world with different preva- lence according to the region. Data derived from the 2009 Population Reference Bureau show that 14% of married women have an IUD. In Australia this figure is only less than 2% [1].
IUDs are considered both safe and effective [2]. However, there are several possible complications associated with their use. These include the increased risk of infection, dysmenorrhea, hypermenorrhoea, pelvic infection, pregnancy, septic abortion, uterine perforation and migration into adjacent organs [3]. The latter two will be the subjects of this case study.
Uterine perforation is the most serious complication of the IUD placement, occurring in 1.6 per 1000 insertions. Most perforations and consequent translocations are thought to be associated with the insertion procedure [4]. When a perforation occurs, it is most commonly seen through the posterior wall of the uterus. Patients may be asymptomatic or present with tenderness, fibrosis and adhesion formation. Exceptionally, other intra-abdominal organs are injured [5].
It has been described that IUDs can cause perforation of the caecum and sigmoid colon, appendix and small bowel and less commonly the ovaries, bladder, broad ligament and adnexa [4-7]. The largest study found in the literature reported 23 cases of migrated IUDs over a seven-year period. Only 17% (four cases) were found in the greater omentum with the vast majority presenting asymptomatic at follow-up within three months [8]. However, IUDs can also become embedded in the uterus and with time be forced through the wall into the pelvic or abdominal cavity [8].
The currently accepted treatment for removal of a “lost” IUD is by laparoscopic surgery [9]. Other studies suggest that asymptomatic patients without perforation would benefit from non-operative management. This is because of the morbidity associated with abdominal surgery and general anesthesia [10].
2. CASE REPORT
We describe the case of a 34-year-old woman who presented to her GP with a six-month history of severe right upper quadrant (RUQ) pain, sharp and intermittent, not associated with any other symptoms and clinically suggestive of biliary colic. Whilst waiting for an upper abdominal ultrasound she was received by an Obstetrics and Gynecologist specialist (OG). Four years before, the patient had a Mirena IUD. This time, the coil could not be localized in the uterus on examination. A pelvic US failed to visualize the lost IUD. An abdominal X-ray was then performed (Figure 1). This prompted the patient to have a diagnostic laparoscopy where her specialist where he was unable to retrieve the device due to extensive adhesions to the greater omentum and bowel. A tubal ligation was performed during the same procedure.
Following to this procedure the patient was referred to a General Surgeon who in order to better locate the localization of the migrated IUD organized an abdominopelvic CT-scan. A coronal view of this CT scan confirmed the presence of the IUD in the abdomen (Figure 2). A second look laparoscopy was organized in order to remove the device. The IUD was found in the RUQ wrapped around the greater omentum and trapped between the gallbladder and the transverse colon. The device was safely retrieved using diathermy onto the coil (Figure 3).

Figure 1. Abdominal X-ray of patient showing intrauterine device lodged in the right upper quadrant of the abdomen.
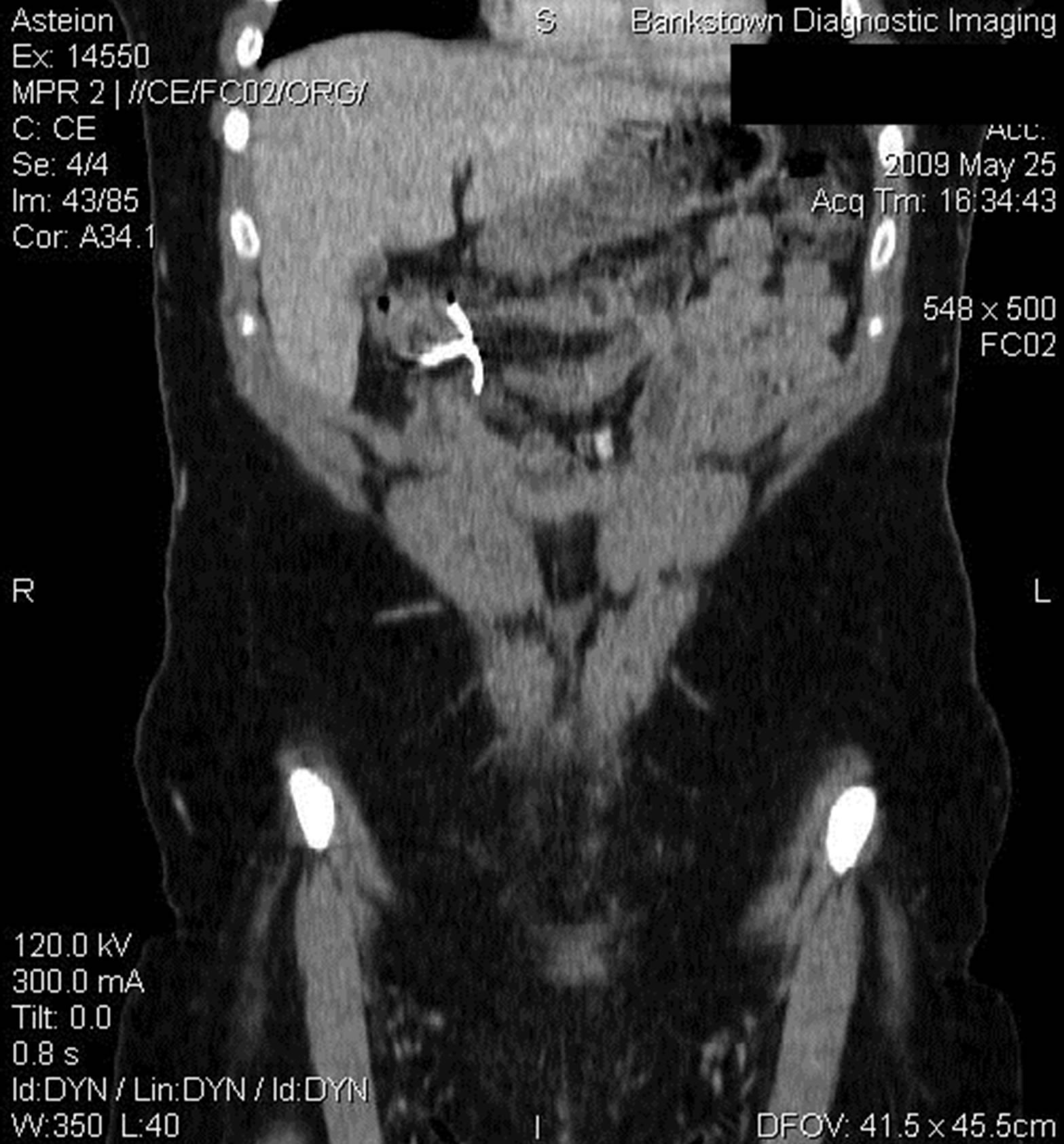
Figure 2. Coronal view of CT Abdomen and pelvis confirming the intrauterine device in right upper quadrant.
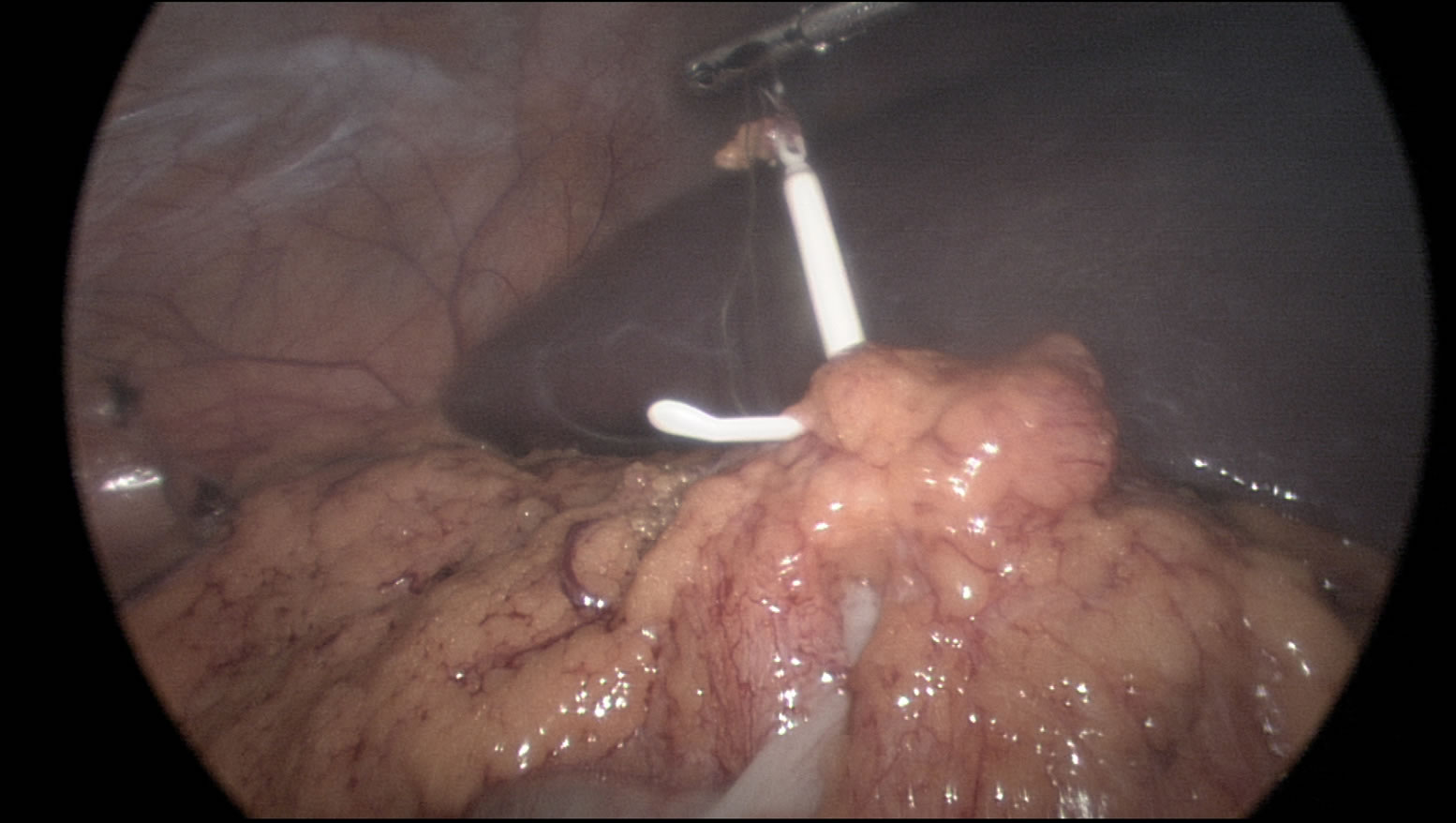
Figure 3. Laparoscopic view of the Intrauterine device wrapped around the greater omentum.
Her post-operative recovery was unremarkable. She was discharged home the next day. At follow up (two and six-weeks) she had no further complains of pain in the right upper abdomen and was fully recovered from the procedure with no complications.
3. DISCUSSION
Our case demonstrates that patients who develop complications after gynecological procedures may present to General Surgeons. We may only encounter these cases rarely since the incidence of perforation and/or migrations of an Intrauterine device are an uncommon complication.
Factors associated with migration such as timing and skill of the proceduralist have been reported [11]. Uterine perforation after insertion of an IUD, has an incidence of 0.12 to 0.68 per 1000 perforations [12] The diagnosis may be delayed for weeks, months and even years.
An important risk factor involved in uterine perforation is the experience of the proceduralist. The insertion of an IUD showed to have higher incidence of migration when performed by a well-trained midwife and compared to medical specialists. During insertion, a higher incidence of migration was detected if occurred within the puerperal period [13]. Our patient is not included in the population at risk since the IUD was both inserted by the OG specialist and not after labour.
In order to prevent the missed diagnosis of this uncommon complication, we and other authors recommend [14] that any patient who has had an IUD inserted should undergo regular self-examination and request medical examination, advice and reassurance in the event of persistent pain. It is important to confirm that the IUD strings are still present in the correct location.
REFERENCES
- The 2009 World Population Data Sheet (2009) Population reference bureau. www.prb.org
- Grimes, D.A., Lopez, L.M., Manion, C. and Schulz, K.F. (2007) Cochrane systematic reviews of IUD trials: Lessons learned. Contraception, 75, S55-S59. doi:10.1016/j.contraception.2006.12.004
- Tinelli, A., Tinelli, R., Malvasi, A., Cavallotti, C. and Tinelli, F.G. (2006) The intrauterine device in modern contraception: Still an actuality? European Journal of Contraception and Reproductive Health Care, 11, 197-201. doi:10.1080/13625180600759755
- Mederos, R., Humaran. L. and Minervini, D. (2008) Surgical removal of an intrauterine device perforating the sigmoid colon: A case report. International Journal of Surgery, 6, e60-e62. doi:10.1016/j.ijsu.2007.02.006
- Sentilhes, L., Lefebvre-Lacoeuille, C., Poilblanc, M. and Descamps, P. (2008) Incidental finding of an intrauterine device in the sigmoid colon. European Journal of Contraception and Reproductive Health Care, 13, 212-214. doi:10.1080/13625180801892868
- Deshmukh, S., Ghanouni, P. and Jeffrey, R.B. (2009) Early sonographic diagnosis of intrauterine device migration to the adnexa. Journal of Clinical Ultrasound, 37, 414-416. doi:10.1002/jcu.20591
- Yensel, U., Bezircioglu, I., Yavuzcan, A., Baloglu, A. and Cetinkaya, B. (2009) Migration of an intrauterine device into the bladder: A rare case. Archives of Gynecology and Obstetrics, 279, 739-742. doi:10.1007/s00404-008-0792-3
- Abdelkerim, Z.B., Mouelhi, C., Chaker, A., Basely, M., Khedher, B., Ferchiou, M., et al. (1997) Laparoscopic surgery of intraperitoneal IUD migration. Study of 23 Cases Tunisie Medicale, 75, 69-71.
- Gupta, I., Sawhney, H. and Mahajan, U. Laparoscopic removal of translocated intrauterine contraceptive devices. Australian and New Zealand Journal of Obstetrics and Gynaecology, 29, 352-355.
- Markovitch, O., Klein, Z., Gidoni, Y., Holzinger, M. and Beyth, Y. (2002) Extrauterine mislocated IUCD: Is surgical removal mandatory? Contraception, 66, 105-108. doi:10.1016/S0010-7824(02)00327-X
- Soydinc, H.E. (2013) Translocated intrauterine contraceptive device: Experiences of two medical centers with risk factors and the need for surgical treatment. Journal of Reproductive Medicine, 58, 234-240.
- Broso, P.R. and Buffetti, G. (1994) The IUD and uterine perforation. Minerva Ginecology, 46, 505-509.
- Harrison-Woolrych, M., Ashton, J. and Coulter, D. (2003) Uterine perforation on intrauterine device insertion: Is the incidence higher than pre previously reported? 67, 53-56.