Journal of Cosmetics, Dermatological Sciences and Applications
Vol.04 No.05(2014), Article ID:51336,6 pages
10.4236/jcdsa.2014.45040
Anti-Inflammatory Efficacy of Product Containing “Skin Calm Complex” in Vitro Reconstructed Epidermis
María Matabuena de Yzaguirre1, Gabriela Bacchini2, Emili Gil Luna2, Eva Vila-Martínez2
1Department of Biology, Faculty of Sciences, Universidad Autónoma de Madrid, Madrid, Spain
2Medical Department, Ferrer Health Care, Barcelona, Spain
Email: maria.matabuena@uam.es
Copyright © 2014 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 28 September 2014; revised 29 October 2014; accepted 4 November 2014
ABSTRACT
Atopic dermatitis is classified as a chronic inflammatory skin disease, which is characterized by alterations in barrier function and immune system of the skin. In a previous study, the efficacy of REPAVAR ATOPIC SKIN BODY CREAM EXTREME (a product containing “SKIN CALM COMPLEX”) on the epidermal barrier structure was demonstrated. However, the product has also been formulated to improve inflammation and itching. The aim of this study is to analyze product effectiveness on skin inflammation and itching which is associated with atopic dermatitis, by quantification of IL-1α and IL-8 interleukins secreted by human keratinocytes from reconstructed epidermis by ELISA assay. Mature (aged 17 days) sample tissues were treated with pro-inflammatory agents (PBS 1X and LPS) and with the product containing synergistic mix from plants extracts and Dihydroavenanthramide D, among other ingredients (“SKIN CALM COMPLEX”) for 24 hours. Measuring the amounts of interleukins by ELISA assay showed 1) decreased levels of IL-1α and 2) no differences about IL-8 secretion. Product REPAVAR ATOPIC SKIN BODY CREAM EXTREME has an anti- inflammatory effect on the release of pro-inflammatory cytokines, becoming an effective preventive agent on inflammation and itching due to maintenance and improvement of the keratinocyte epidermal structure.
Keywords:
Atopic Dermatıtıs, Anti-Inflammatory Effect, In Vitro Assay

1. Introduction
Atopic dermatitis is a chronic inflammatory skin disease, characterized by leukocytes infiltration, alteration of the barrier function of the skin, high rate of water loss, decreased water retention capacity and a lower amount of lipids and ceramides. These events cause uncomfortable symptoms associated with the diseases, such as inflammation and itching, which aggravate the skin condition [1] - [7] .
The etiology of this disease includes interactions between genetic, environmental, epithelial barrier, immune factors and stress [8] - [11] . The results are dry skin, cutaneous hyper-reactivity and inflammation due to cytokine release from lymphocytes, Langerhans cells, keratinocytes, mast cells and eosinophils among the most important cells [12] - [14] . There are data about patients with a genetic profile for a vulnerable epithelial barrier, which pro- vokes an altered immune response and inflamed skin. In this context, epidermis plays a fundamental role in the etiology and development of atopic dermatitis. When the epithelial barrier functions are damaged, inflammatory events and sensitization processes IgE mediated occurs. So epidermis is not only a physical barrier, but also a chemical and immune barrier [15] . In addition, itch-scratch cycle exacerbates the epidemic barrier damage, increases water loss, dryness and inflammation, and favors pathogenic infections of the skin [1] [16] . On the other case, in which external factors alter barrier function, a complex process triggers involving resident epidermal cells: keratinocytes, dermal fibroblasts, endothelial cells and leukocytes interacting with each other under the control of cytokine type mediators and lipids. When the epidermal barrier is impaired, keratinocytes secrete IL- 1α and pro-inflammatory cytokine that induce production of IL-8 (chemo-attractant cytokine). IL-8 recruits immune system cells which secrete interleukins associated with pruritus and specific inflammation, such as IL- 31 in T cells [3] [4] [17] [18] .
In a previous study, the efficacy of the REPAVAR ATOPIC SKIN BODY CREAM EXTREME (a product containing “SKIN CALM COMPLEX”) on the improving the structure and the epidermal barrier was demonstrated. However, this complex product also contains ingredients to act on inflammation and itching. The study of anti-inflammatory potential was carried out in reconstructed human epithelium model (3D). However, these reconstructed human epithelia lack immune and nervous system cells from human skin [19] . So only the effect of the product on interleukins secreted by keratinocytes was analyzed.
The aim of this work was to confirm the anti-inflammatory action of the REPAVAR ATOPIC SKIN BODY CREAM EXTREME product containing ingredients of the “SKIN CALM COMPLEX” whose effectiveness was demonstrated separately.
2. Methods
2.1. In Vitro Model
In vitro Reconstructed Human Epidermis of 0.33 cm2, aged 17 days (28 samples), produced by SkinEthic laboratories (Nice, France) were used (for more information visit SkinEthic website [19] ). The tissues were cultured and kept in chemically defined medium, provided by the same laboratory, during the assays. Tissue cultures were performed in an incubator with 5% of CO2 at 37˚C. The tissue manipulation process was carried out in sterile conditions.
2.2. Treatments
4 samples per group were used: i) Negative control (-SkinEthic Maintenance Medium- SkinEthic laboratories, Nice, France); ii) IL-1α inflammation positive control (phosphate buffered saline, PBS 1X, -HyClone Laboratories, Inc., South Logan, UT-, for 4 hours + maintenance medium for 24 hours); iii) IL-8 inflammation positive control (Escherichia coli LPS 100 μg/ml -Sigma, St. Louis, MO- diluted in maintenance medium, for 24 hours); iv) IL-1α anti-inflammation positive control (PBS 1X, for 4 hours + 10 μM Dexamethasone -Sigma, St. Louis, MO-, diluted in maintenance medium, for 24 hours); v) IL-8 anti-inflammation positive control (LPS 100 μg/ml + 10 μM Dexamethasone, diluted in maintenance medium, for 24 hours); vi) IL-1α inflammation treatment + Product (PBS 1X, for 4 hours + “REPAVAR ATOPIC SKIN BODY CREAM EXTREME”, for 24 hours); vii) IL-8 inflammation treatment + Product (LPS 100 μg/ml diluted in maintenance medium + “REPAVAR ATOPIC SKIN BODY CREAM EXTREME”, for 24 hours).
2.3. MTT Assay
Cellular viability was assessed by MTT (3-[4,5-dimethylthiazol-2-yl]-2,5 diphenyltetrazolium bromide) assay (Sigma, St. Louis, MO), a method based on the activity of mitochondrial dehydrogenases [20] . Stock solution of MTT (5 mg/ml) in PBS, was diluted (1 mg/ml) in SkinEthic culture medium, and then the samples were incubated at 37˚C, 5% CO2, 95% humidified atmosphere, for 3 hours. The resulting formazan crystals were dissolved by the addition of isopropanol (Sigma, St. Louis, MO), at room temperature, for 2 hours with gentle agitation. Optical Densities (OD) were measured at 570 nm wavelength.
2.4. Immunodetection by ELISA
The release of interleukin in the supernatants from keratinocytes was determined using the ELISA kit for IL-1α (Abcam, Cambridge, UK) and IL-8 (Abcam, Cambridge, UK), following the manufacturer’s instructions.
In both cases, the reading of the optical density (OD) was carried out at 450 nm against the blank (diluent).
2.5. Statistical Analysis
The statistical analysis was performed using the SPSS 15.0, 1 software (SPSS Inc., Chicago, IL), using Student’s t test and analysis of variance (ANOVA), and considering a p < 0.05 as statistically significant.
3. Results and Discussion
3.1. Production of IL-1α
IL-1α is a pleiotropic cytokine implicated in inflammation, immune responses and cell differentiation processes, which increases in response to cell damage, inducing apoptosis. In this study, culture maintenance medium was replaced by PBS for 4 hours, to promote disintegration of the epidermal barrier and to check the existence of any relationship between epithelial integrity and swelling.
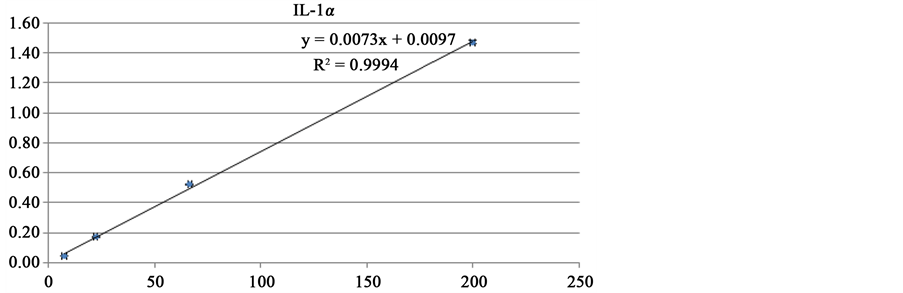
Standard curve were calculated from DO readings at 450 nm and known protein concentration (pg/ml) (Figure 1(a)). Then, production of IL-1α data were calculated for each of the treatment groups.
Means of interleukin release was compared (Figure 1(b)) and statistical analysis data showed significant differences (p < 0.05) among the negative control group and positive control inflammation (PBS 1X, p = 0.0268) and between the negative control and positive control anti-inflammation (PBS 1X + Dexamethasone, p = 0.0017), although a notable reduction on IL-1α secretion was detected in this last situation. However, when comparing the groups negative control vs. PBS 1X + Product, p value was >0.05 (p = 0.1), indicating that the differences between them are not significant. Therefore, it is confirmed the product “REPAVAR ATOPIC SKIN BODY CREAM EXTREME” effect on inflammation mediated by IL-1α, in response to barrier damage.
Extrapolation of inhibiting release of IL-1α in the sample treated with the product “REPAVAR ATOPIC SKIN BODY CREAM EXTREME” was calculated as the percentage of reducing the amount of protein released, relative to positive control anti-inflammatory (PBS 1X + Dexamethasone), having subtracted the value of production of IL-1α negative control. As shown in Figure 1(c), the product “REPAVAR ATOPIC SKIN BODY CREAM EXTREME” seems to prevent the release of IL-1α.
3.2. Production of IL-8
Since IL-8 is a chemotactic factor, implicated in the attraction and activation of immune cells, produced by keratinocytes in response to inflammatory stimuli, LPS was used to induce the production of this protein.
Following a similar procedure, when comparing LPS positive control group against inflammation treatment IL-8 + Product, p value was >0.05 (p = 0.15), indicating that the differences between them are not significant (data not shown). So that, product “REPAVAR ATOPIC SKIN BODY CREAM EXTREME” shows no effect on the release of IL-8.
Analysis of cell viability was included in the experiments as control treatments and data were not shown normally. But in the case of IL-8, surprisingly, meanwhile the positive controls (LPS and LPS + Dexamethasone) showed cell viability values around 80% compared to negative control (maintenance medium), implying the treatments are well tolerated by tissues, the Product-treated sample shows an increase of 35% compared to untreated tissue (negative control), reflecting that effect on epithelial regeneration processes (Figure 2).
These results are consistent with data previously obtained [21] . Product “REPAVAR ATOPIC SKIN BODY CREAM EXTREME”-treated tissues showed an increase in the number of cells and an improvement in the epithelial morphology and the expression of structural proteins.
Nowadays, treatments for dermatological diseases characterized by an altered immune response, involving inflammation and itching, as atopic dermatitis, include emollients to increase hydration levels and topical corti-
 (a)
(a)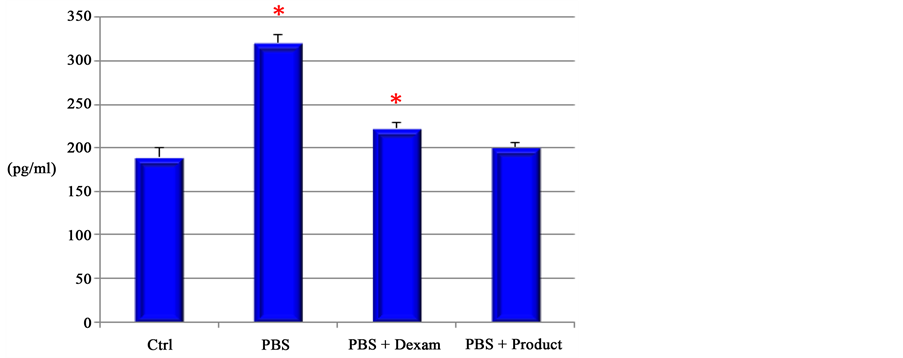 (b)
(b)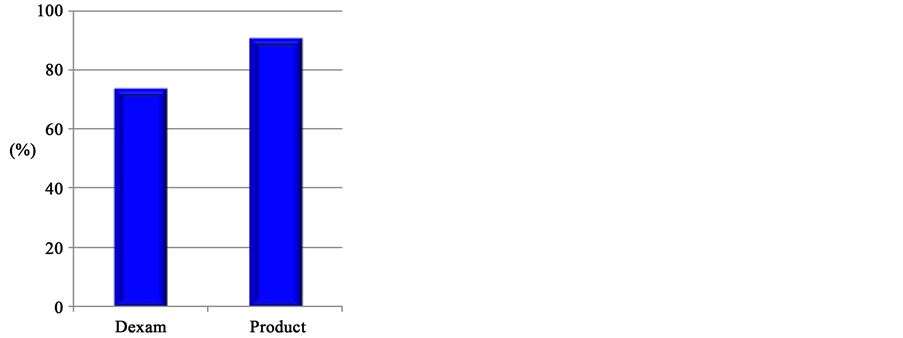 (c)
(c)
Figure 1. (a) IL-1α Standard Curve. The R value (regression) is reliable, because it is close to X axis, protein concentrations (pg/ml); Y axis, absorbance (450 nm). (b) Release of IL-1α. Ctrl, untreated tissues; PBS, positive control inflammation; PBS + Dexamethasone, positive control anti-inflammation; PBS + Product (“ATOPIC SKIN BODY CREAM EXTREME”). The product exerts an anti-inflammatory effect in the case of IL-1α. (c) Inhibition of IL-1α induced by Dexamethasone (Dexam) and “ATOPIC SKIN BODY CREAM EXTREME EXTREME BODY CREAM SKIN ATOPIC” (Product). “ATOPIC SKIN BODY CREAM EXTREME EXTREME BODY CREAM SKIN ATOPIC”-treated samples present a 90% of inhibition in IL- 1α levels, while the Dexamethasone’s efficiency is about 70%.
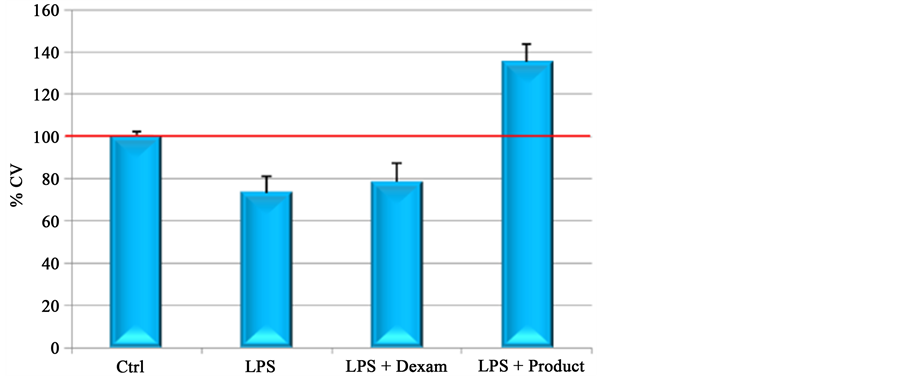
Figure 2. Cell viability (% CV). Ctrl, untreated tissues; LPS, positive control of inflammation; LPS + dexamethasone, positive control of anti-inflammation; LPS + Product (“ATOPIC SKIN BODY CREAM EXTREME”). Product- treated sample shows an increase in cell viability of about 35% respecting un- treated tissues.
costeroids associated with adverse side effects [22] [23] . At present, research focuses on the search and combination of more effective new agents with the least side effects. The product used in this study (“ATOPIC SKIN BODY CREAM EXTREME”) contains “SKIN CALM COMPLEX”, which includes, among other ingredients, a multi-herbal complex extracted from seven plants (Rosemarinus officinalis, Matricaria recubita, Camellia sinensis, Glycyrrhiza glabra, Polygonum cuspidatum, Scutellaria baicalensis and Centella asiatica) and Dihydroavenanthramide D, synthetic Avenanthramide. Both active ingredients have shown their efficacy in the treatment of atopic dermatitis: i) multicompound herbal preparation showed anti-inflammatory effects by reduction of IL-8 production in vitro by lymphocytes and monocytes, and reduction of eczema area severity index (EASI), degree of pruritus and TEWL [24] ; ii) keratinocytes treated with Avenanthramides showed a reduction of IL-8 release in vitro and topical application in murine models mitigated inflammation and pruritogen-induced scratching [25] . In this study, no effect on the production of IL-8 was found. This fact may be due to the action of Avenanthramides in the product is not as straightforward as when acting in isolation.
However, data obtained from quantization of pro-inflammatory cytokine IL-1α, by ELISA assay, demonstrate the anti-inflammatory effect of the product “REPAVAR ATOPIC SKIN BODY CREAM EXTREME” by topical application in reconstructed human epidermis. Other authors postulate thatkeratinocytes aretargets of T lymphocytes infiltrating immune processes, to have an active role in atopic dermatitis. Its role in maintaining homeostasis and proper functionality of the skin is essential not only for the correct expression of proteins that ensure epithelial structure, but for the production of lipids that prevent the loss of water and production of cytokines involved in activation and cell chemotaxis processes (inflammation), in proliferation and differentiation [26] [27] .
4. Conclusion
This study demonstrates that the product may be highly effective in mild atopic dermatitis and the early stage of a moderate/severe illness. It improves the epidermal barrier effect and prevents inflammation, although studies in patients will be needed to confirm this hypothesis.
References
- Boguniewicz, M. and Leung, D.Y. (2011) Atopic Dermatitis: A Disease of Altered Skin Barrier and Immune Dysregulation. Immunological Reviews, 242, 233-246. http://dx.doi.org/10.1111/j.1600-065X.2011.01027.x
- Kasraie, S. and Werfel, T. (2013) Role of Macrophages in the Pathogenesis of Atopic Dermatitis. Mediators of Inflammation, 2013, 1-15. http://dx.doi.org/10.1155/2013/942375
- Segre, J.A. (2006) Epidermal Barrier Formation and Recovery in Skin Disorders. The Journal of Clinical Investigation, 116, 1150-1158. http://dx.doi.org/10.1172/JCI28521
- Jensen, L.E. (2010) Targeting the IL-1 Family Members in Skin Inflammation. Current Opinion in Investigational Drugs, 11, 1211-1220.
- Engelhart, K., El Hindi, T., Biesalski, H.K. and Pfitzner, I. (2005) In Vitro Reproduction of Clinical Hallmarks of Eczematous Dermatitis in Organotypic Skin Models. Archives of Dermatological Research, 297, 1-9. http://dx.doi.org/10.1007/s00403-005-0575-7
- Tivoli, Y.A. and Rubenstein, R.M. (2009) Pruritus: An Updated Look at an Old Problem. Journal of Clinical and Aesthetic Dermatology, 2, 30-36.
- Steinhoff, M., Bienenstock, J., Schmelz, M., Maurer, M., Wei, E. and Bíró, T. (2006) Neurophysiological, Neuroimmunological, and Neuroendocrine Basis of Pruritus. Journal of Investigative Dermatology, 126, 1705-1718. http://dx.doi.org/10.1038/sj.jid.5700231
- Pastar, Z., Lipozencić, J. and Ljubojević, S. (2005) Etiopathogenesis of Atopic Dermatitis—An Overview. Acta Dermatovenerologica Croatica, 13, 54-62.
- Polo, N. (2003) Dermatitis atópica. JANO, 1.475, 42-44.
- Novak, N. and Leung, D.Y. (2011) Advances in Atopic Dermatitis. Current Opinion in Immunology, 23, 778-783. http://dx.doi.org/10.1016/j.coi.2011.09.007
- Elias, P.M. (2010) Therapeutic Implications of a Barrier-Based Pathogenesis of Atopic Dermatitis. Annals of Derma- tology, 22, 245-254. http://dx.doi.org/10.5021/ad.2010.22.3.245
- Ballona, R. and Ballona, C. (2004) Dermatitis atópica. Folia Dermatológica Peruana, 15, 40-48.
- Theoharides, T.C., Alysandratos, K.D., Angelidou, A., Delivanis, D.A., Sismanopoulos, N., Zhang, B., Asadi, S., Vasiadi, M., Weng, Z., Miniati, A. and Kalogeromitros, D. (2012) Mast Cells and Inflammation. Biochimica et Biophysica Acta, 1822, 21-33.
- Elias, P.M. and Schmuth, M. (2009) Abnormal Skin Barrier in the Etiopathogenesis of Atopic Dermatitis. Current Allergy and Asthma Reports, 9, 265-272. http://dx.doi.org/10.1007/s11882-009-0037-y
- Komine, M. (2009) Analysis of the Mechanism for the Development of Allergic Skin Inflammation and the Application for Its Treatment: Keratinocytes in Atopic Dermatitis—Their Pathogenic Involvement. Journal of Pharmacological Sciences, 110, 260-264. http://dx.doi.org/10.1254/jphs.09R06FM
- Klein, P.A. and Clark, R.A. (1999) An Evidence-Based Review of the Efficacy of Antihistamines in Relieving Pruritus in Atopic Dermatitis. JAMA Dermatology, 135, 1522-1525. http://dx.doi.org/10.1001/archderm.135.12.1522
- Brandt, E.B. and Sivaprasad, U. (2011) Th2 Cytokines and Atopic Dermatitis. Journal of Clinical & Cellular Immunology, 2, 110-123. http://dx.doi.org/10.4172/2155-9899.1000110
- Sonkoly, E., Muller, A., Lauerma, A.I., Pivarcsi, A., Soto, H., Kemeny, L., Alenius, H., Dieu-Nosjean, M.C., Meller, S., Rieker, J., Steinhoff, M., Hoffmann, T.K., Ruzicka, T., Zlotnik, A. and Homey, B. (2006) IL-31: A New Link between T Cells and Pruritus in Atopic Skin Inflammation. Journal of Allergy and Clinical Immunology, 117, 411-417. http://dx.doi.org/10.1016/j.jaci.2005.10.033
- http://www.skinethic.com/RHE.asp
- Merlin, J.L., Azzi, S., Lignon, D., Ramacci, C., Zeghari, N. and Guillemin, F. (1992) MTT Assays Allow Quick and Reliable Measurement of the Response of Human Tumour Cells to Photodynamic Therapy. European Journal of Cancer, 28, 1452-1458. http://dx.doi.org/10.1016/0959-8049(92)90542-A
- Matabuena-de Yzaguirre, M., Bacchini, G., Vila-Martínez, E. and Juarranz, A. (2014) Product Containing “Skin Calm Complex” Improves Barrier Effect in Vitro. Journal of Cosmetics, Dermatological Sciences and Applications, 4, 234- 243. http://dx.doi.org/10.4236/jcdsa.2014.44032
- Venge, P. (1993) Eosinophil and Neutrophil Granulocytes. Allergy, 48, 39-47. http://dx.doi.org/10.1111/j.1398-9995.1993.tb04697.x
- Hong, J., Buddenkotte, J., Berger, T.G. and Steinhoff, M. (2011) Management of Itch in Atopic Dermatitis. Seminars in Cutaneous Medicine and Surgery, 30, 71-86. http://dx.doi.org/10.1016/j.sder.2011.05.002
- Lee, J., Jung, E., Park, B., Jung, K., Park, J., Kim, K., Kim, K.H. and Park, D. (2005) Evaluation of the Anti-Inflammatory and Atopic Dermatitis-Mitigating Effects of BSASM, a Multicompound Preparation. Journal of Ethnopharmacology, 96, 211-219. http://dx.doi.org/10.1016/j.jep.2004.09.012
- Sur, R., Nigam, A., Grote, D., Liebel, F. and Southall, M.D. (2008) Avenanthramides, Polyphenols from Oats, Exhibit Anti-Inflammatory and Anti-Itch Activity. Archives of Dermatological Research, 300, 569-574. http://dx.doi.org/10.1007/s00403-008-0858-x
- Albanesi, C., Scarponi, C., Giustizieri, M.L. and Girolomoni, G. (2005) Keratinocytes in Inflammatory Skin Diseases. Current Drug Target-Inflammation & Allergy, 4, 329-334. http://dx.doi.org/10.2174/1568010054022033
- Uchiyama, N., Yamamoto, A., Kameda, K., Yamaguchi, H. and Ito, M. (2000) The Activity of Fatty Acid Synthase of Epidermal Keratinocytes Is Regulated in the Lower Stratum Spinousum and the Stratum Basale by Local Inflammation Rather than by Circulating Hormones. Journal of Dermatological Science, 24, 134-141. http://dx.doi.org/10.1016/S0923-1811(00)00088-8