F. C. B. ABDALLAH ET AL.
Copyright © 2012 SciRes. OJRD
59
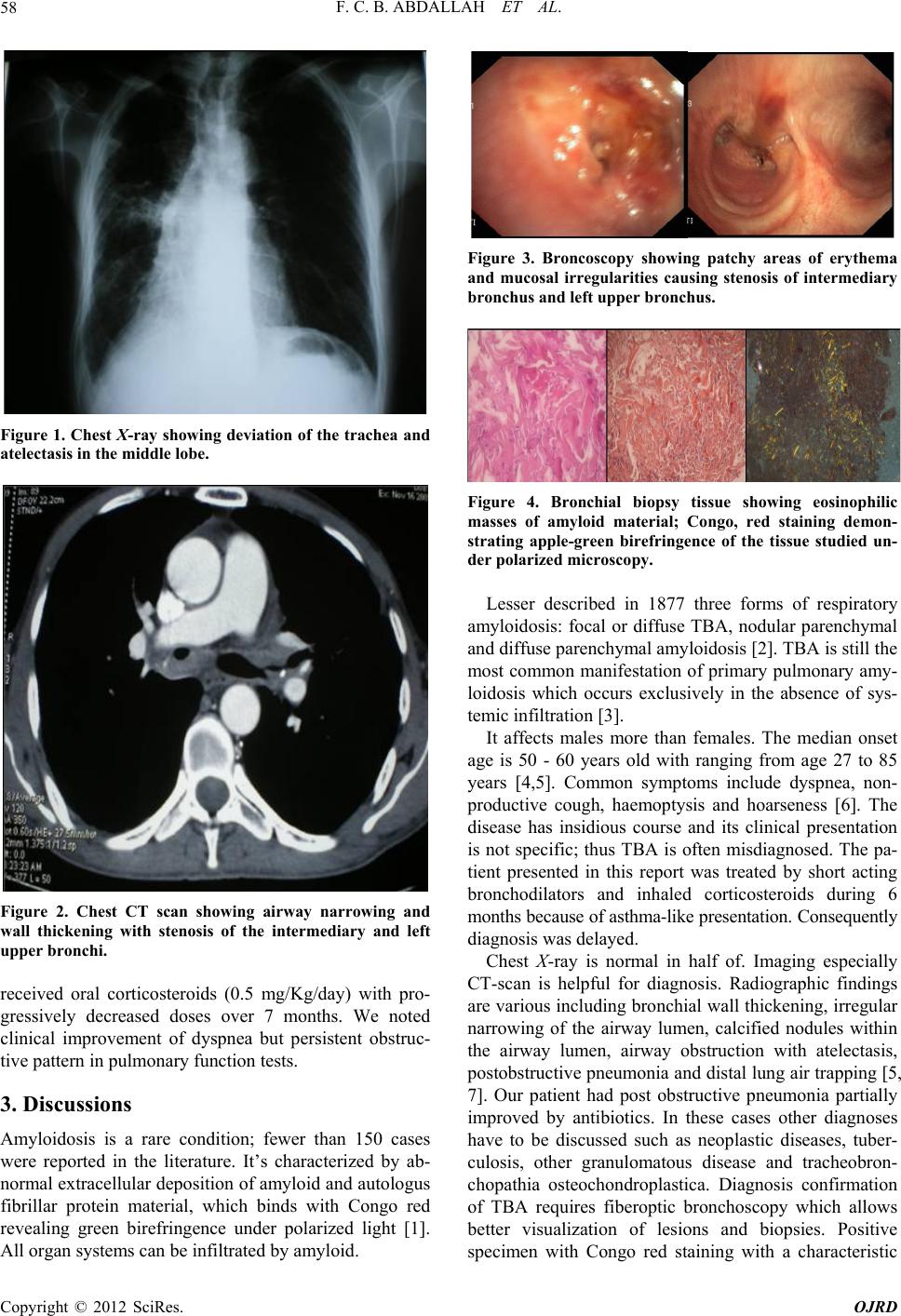
apple green birefringence with polarized light is the
proof of amyl oidosis di sease [ 4, 5].
The treatment of localized TBA is essentially symp-
tomatic [8]. Strategies depend on the site and extent of
the disease. In fact, only observation can be indicated in
asymptomatic patients. However, local and or systemic
therapies are recommended in patients with severe air-
way obstruction [9]. Drugs inhibiting the synthesis,
deposition and degradation of amyloid in tissues, espe-
cially colchicine, prednisone and melphalan were used
but with a limited effect [4,9]. Varied methods of bron-
choscopic treatment have been reported such as endo-
bronchial Nd-YAG laser, tracheobronchial stents, bal-
loon dilation and bronchoscopic ablation of intraluminal
amyloid deposits. These methods are associated with a
risk of bleeding and recurrences [4]. Surgery may be
necessary when airway involvement is extensive [5]. Re-
cently, some investigators demonstrated that external
beam radiation therapy (EBRT) may provide an objective
improvement [10]. Also M. Truong found in his study
that EBRT prevents progressive amyloid deposition in
90% of patients with localized airway amyloidosis and it
is well tolerated with minimal toxicity [11].
Although TBA is a localized process, it is associated
with poorer prognosis. Authors reported that overall sur-
vival ranges from 31% to 43% at 4 to 6 years. In absence
of curative treatment of TBA, researchers are still con-
tinuously trying o ther therapeutic alternatives to improve
the prognosis of these patients.
4. Conclusion
Diagnosis of TBA has to be considered in patients with
asthma-like dyspnea in whom anti-asthmatic treatments
are ineffective. The diagnosis can be suggested by radio-
graphic findings but it is confirmed essentially through
bronchoscopic biopsies, with appropriate Congo red
staining of the bronchial tissue samples obtained. At
present, there are no therapeutic options proved to be
completely successful. However, bronchoscopic man-
agement often proves to be temporarily effective, while
EBRT still need to be further evaluated. Prognosis of
TBA remains poor.
REFERENCES
[1] H. Gibbaoui, S. Abouchacra and M. Yaman, “A Case of
Primary Diffuse Tracheobronchial Amyloidosis,” The
Annals of Thoracic Surgery, Vol. 77, No. 5, 2004, pp.
1832-1834. doi:10.1016/S0003-4975(03)00999-8
[2] A. Lesser, “Ein Fall von Enchondroma Osteiodes Mixtum
der Lunge Mit Partieller Amyloid Entortung,” Virchows
Archiv , Vol. 69, No. 3-4, 1877, pp. 404-409.
doi:10.1007/BF02326214
[3] C. Ozer, M. N. Duce, A. Yildiz, F. D. Apaydin, H. Egil-
mez and T. Arpaci, “Primary Diffuse Tracheobronchial
Amyloidosis: Case Report,” European Journal of Radi-
ology, Vol. 44, No. 1, 2002, pp. 37-39.
doi:10.1016/S0720-048X(01)00437-5
[4] H. Mao, X. Yang, Z. Wang, X. Chen and Q. Yi, “Asthma-
Like Tracheobronchial Amyloidosis: A Case Report and
Review of the Literature,” Journal of Nanjing Medical
University, Vol. 22, No. 5, 2008, pp. 317-322.
doi:10.1016/S1007-4376(08)60088-X
[5] K. A. Dahl, K. H. Kernstine, T. L. Vannatta, M. W.
Karwal, K. W. Thomas and D. F. Schraith, “Tracheo-
bronchial Amyloidosis: A Surgical Disease with Long-
Term Consequences,” Journal of Thoracic Cardiovascu-
lar Surgery, Vol. 128, No. 5, 2004, pp. 789-792.
[6] A. T. Monroe, R. Walia, R. A. Zlotecki and M. A. Jantz,
“Tracheobronchial Amyloidosis: A Case Report of Suc-
cessful Treatment with External Beam Radiation Ther-
apy,” Chest, Vol. 125, No. 2, 2004, pp. 784-789.
doi:10.1378/chest.125.2.784
[7] J. W. Santos, A. S. Filho, A. Bertolazzi, G. T. Michel, L.
V. Silva, C. R. Melo, V. D. Pedro, D. Spilmann and J. K.
Figaro, “Amyloidosis Tracheobronchial Primary,” Jour-
nal Brasileiro Pneumologia, Vol. 34, No. 10, 2008, pp.
881-884. doi:10.1590/S1806-37132008001000015
[8] A. K. Brill, K. Woelke, R. Schadlich, C. Weinz and G. Laier-
Gr oe neveld, “Tracheobronchial Amyloidosis-Bronchoscopic
Diagnosis and Therapy of an Uncommon Disease: A Case
Report,” Journal of Physiology and Pharmacology, Vol.
58, No. 5, 2007, pp. 51-55.
[9] H. C. Chew, S. Y. Low, P. Eng, T. Agasthian and F. K.
Cheah, “Cough and Persistant Wheeze in a Patient with
Long-Standing Asthma,” Chest, Vol. 132, No. 2, 2007, pp.
727-731. doi:10.1378/chest.06-2810
[10] M. A. Neben-Wittich, R. L. Foote and S. Kalra, “External
Beam Radiation Therapy for Tracheobronchial Amyloi-
dosis,” Chest, Vol. 132, No. 1, 2007, pp. 262-267.
doi:10.1378/chest.06-3118
[11] M. Truong, L. A. Kachnic, G. A. Grillone and J. L. Berk,
“The Role of Radiation Therapy for Progressive Airway
Amyloidosis,” International Journal of Radiation On-
cology Biology Physics, Vol. 69, No. 3, 2007, p. S122.
doi:10.1016/j.ijrobp.2007.07.226