 Creative Education 2012. Vol.3, No.2, 263-268 Published Online April 2012 in SciRes (http://www.SciRP.org/journal/ce) http://dx.doi.org/10.4236/ce.2012.32041 Copyright © 2012 SciRe s . 263 Health of School-Aged Children in 11+ Hours of Center-Based Care Tokie Anme1, Ryoji Shinohara1, Yuka Sugisawa1, Lian Tong1, Emiko Tanaka1, Etsuko Tomisaki1, Taeko Watanabe1, Kentaro T o kut ake1, Yukiko Mot i z u k i 1, Hisako Matsumoto1, Chihiro Sugita1, Uma Segal2 1Graduate School of Comprehensive Human Sciences, University of Tsukuba, Tsukuba, Japan 2School of Social Work, University of Missouri, St. Louis, USA Email: anmet@md.tsukuba.ac.jp Received March 18th, 2012; revised April 12th, 2012; accepted April 28th, 2012 With increasing numbers of women joining the evening/nighttime and extended-hour workforce, there is a need for quality childcare during these hours. This project, conducted in Japan, sought to compare the effects of expanded child-care on the health of 271 school-aged children. Parents completed a survey on the childrearing environment at home, their feelings of self-efficacy, and the presence of support for childcare; and childcare professionals evaluated the development of these school-aged children. Children responded to questions regarding their health. Results of the multiple regression analysis indicate that factors in the home environment, not length of time in center-based care, explained health risks at school age. Keywords: Health; Child-Care; Cohort Study Introduction Demands for the expansion of center-based child night and extended-hour care have dramatically increased with the rising numbers of working mothers in Japan. High-quality center- based night care is essential to provide a safe and comfortable environment for children whose parents are employed in occu- pations that require long hours including evening and night shifts. Sixty-one authorized night care facilities, centers that are licensed by the national government as meeting quality care standards, have been established since 1981, after the several highly publicized involuntary homicides (cases of neglectful death) in the existing low-quality “Baby Hotels”. Baby Hotels are facilities that continue to exist in Japan and that provide childcare services 24 hours-a-day for children from birth to seven years of age. With the continued shortage of authorized facilities, over 120,000 children use non-authorized, sub-stan- dard Baby Hotels (Anme & Segal, 2003, 2004). Governmental authorization standards are high, including many criteria in- cluding child-to-professional ratios (three babies to one nation- ally licensed professional), credentialling (licensed child care professionals and nurses), adequacy of physical environment (space, facilities, safety assurance) and sound management (budget, accountability, oversight). The community health program that allows visiting nurses to provide preventative care for children in the home ceases as children enter the formal educational system, and primary schools experience a growing problem with increasing numbers of students with rising health concerns. Japanese children can be in child care from the ages 4 months to six years, the period during which they receive home visits from community nurses. They attend primary school (grades one to six) from seven years of age to twelve yeas. After six years in primary school, all children proceed to junior high school for another three years. Over 96% of these children go on to senior high shool for three more years, and 2006 census reports indicate that 76% children get higher education at a university or college follow- ing high school. It is essential that the health of these children be assessed to prevent health decline and to promote health for children in the school system. Longitudinal research from the United Kingdom (1958-2007), and others, indicates the importance of the child environment during the toddler years in predicting later development (Shoon, 2006; Shoon & Parson, 2002; Sacker, 2002; Salmela-Aro, 2005). The quality of care must be considered carefully if the effects of early childcare are to be understood [National Insti- tute of Child Health and Human Development (NICHD), 1999a]. Children from higher-quality centers have been found to be less anxious and have less problematic transitions to school. However, in another longitudinal study, such positive effects of high quality center care facilities were not discernible among all children sampled at age 13 years (Andersson, 1992). NICHD (2001, 2002a) further found that the quality of maternal caregiving was the strongest predictor of development but that the quality of nonmaternal caregiving was also associated with children’s development. Contrary to the NICHD’s expectations, however, family risk factors were the strongest predictors of behavior problems, prosocial behavior, and langauge skills in another longitudinal study, but there was limited evidence that child care experiences moderated the negative associations between family risk and the child outcomes under investigation (NICHD, 2002b). The NICHD (2003) and Langlois and Liben (2003) arrived at three conclusions: 1) the cumulative quantity of child care dur- ing the first four years of life predicts some problematic beha- viors of children between ages 4.5 and 5 years, but these be- haviors were corroborated by reports of parents and teachers, 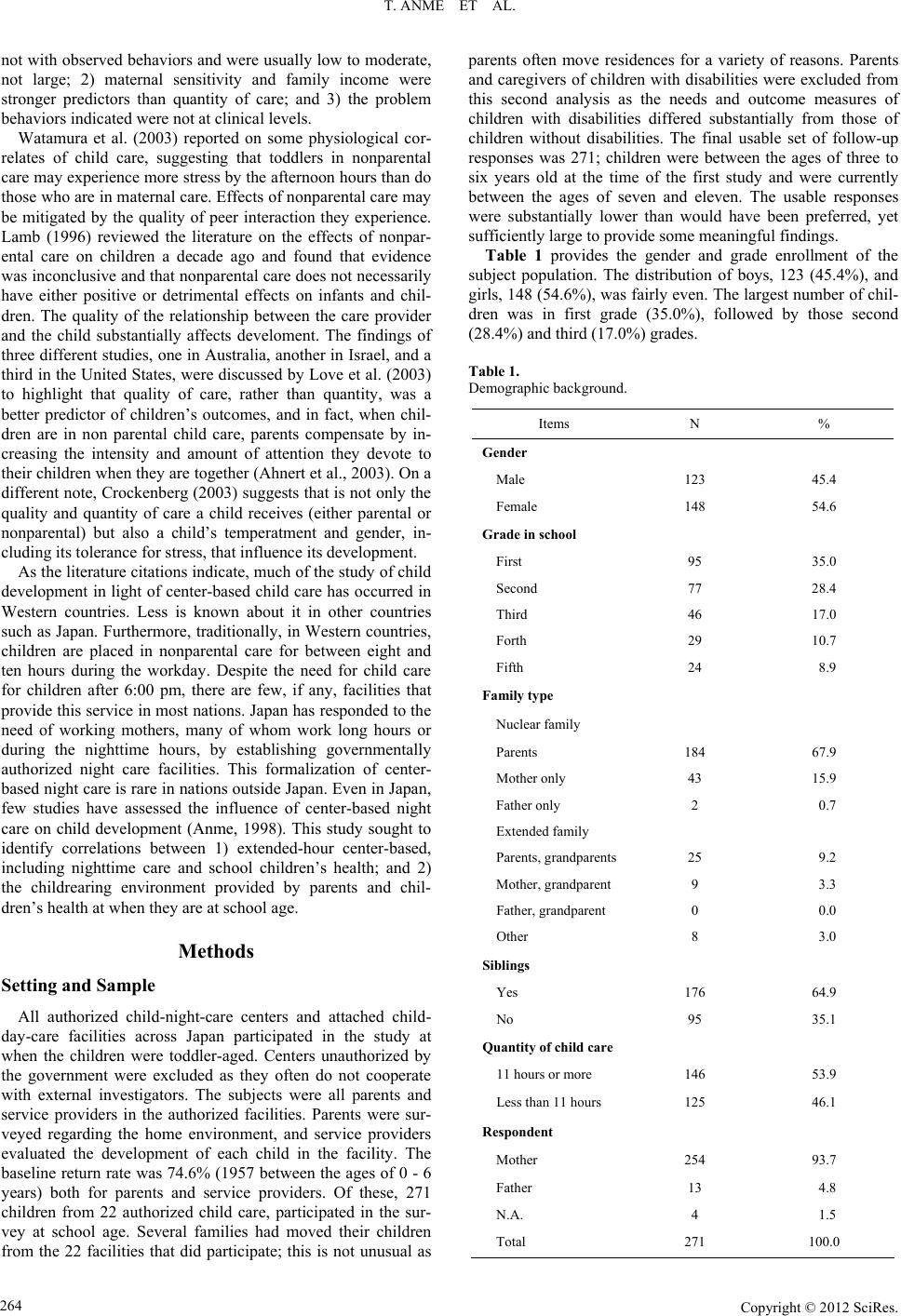 T. ANME ET AL. not with observed behaviors and were usually low to moderate, not large; 2) maternal sensitivity and family income were stronger predictors than quantity of care; and 3) the problem behaviors indicated were not at clinical levels. Watamura et al. (2003) reported on some physiological cor- relates of child care, suggesting that toddlers in nonparental care may experience more stress by the afternoon hours than do those who are in maternal care. Effects of nonparental care may be mitigated by the quality of peer interaction they experience. Lamb (1996) reviewed the literature on the effects of nonpar- ental care on children a decade ago and found that evidence was inconclusive and that nonparental care does not necessarily have either positive or detrimental effects on infants and chil- dren. The quality of the relationship between the care provider and the child substantially affects develoment. The findings of three different studies, one in Australia, another in Israel, and a third in the United States, were discussed by Love et al. (2003) to highlight that quality of care, rather than quantity, was a better predictor of children’s outcomes, and in fact, when chil- dren are in non parental child care, parents compensate by in- creasing the intensity and amount of attention they devote to their children when they are together (Ahnert et al., 2003). On a different note, Crockenberg (2003) suggests that is not only the quality and quantity of care a child receives (either parental or nonparental) but also a child’s temperatment and gender, in- cluding its tolerance for stress, that influence its development. As the literature citations indicate, much of the study of child development in light of center-based child care has occurred in Western countries. Less is known about it in other countries such as Japan. Furthermore, traditionally, in Western countries, children are placed in nonparental care for between eight and ten hours during the workday. Despite the need for child care for children after 6:00 pm, there are few, if any, facilities that provide this service in most nations. Japan has responded to the need of working mothers, many of whom work long hours or during the nighttime hours, by establishing governmentally authorized night care facilities. This formalization of center- based night care is rare in nations outside Japan. Even in Japan, few studies have assessed the influence of center-based night care on child development (Anme, 1998). This study sought to identify correlations between 1) extended-hour center-based, including nighttime care and school children’s health; and 2) the childrearing environment provided by parents and chil- dren’s health at when they are at school age. Methods Setting and Sample All authorized child-night-care centers and attached child- day-care facilities across Japan participated in the study at when the children were toddler-aged. Centers unauthorized by the government were excluded as they often do not cooperate with external investigators. The subjects were all parents and service providers in the authorized facilities. Parents were sur- veyed regarding the home environment, and service providers evaluated the development of each child in the facility. The baseline return rate was 74.6% (1957 between the ages of 0 - 6 years) both for parents and service providers. Of these, 271 children from 22 authorized child care, participated in the sur- vey at school age. Several families had moved their children from the 22 facilities that did participate; this is not unusual as parents often move residences for a variety of reasons. Parents and caregivers of children with disabilities were excluded from this second analysis as the needs and outcome measures of children with disabilities differed substantially from those of children without disabilities. The final usable set of follow-up responses was 271; children were between the ages of three to six years old at the time of the first study and were currently between the ages of seven and eleven. The usable responses were substantially lower than would have been preferred, yet sufficiently large to provide some meaningful findings. Table 1 provides the gender and grade enrollment of the subject population. The distribution of boys, 123 (45.4%), and girls, 148 (54.6%), was fairly even. The largest number of chil- dren was in first grade (35.0%), followed by those second (28.4%) and third (17.0%) grades. Table 1. Demographic background. Items N % Gender Male 123 45.4 Female 148 54.6 Grade in school First 95 35.0 Second 77 28.4 Third 46 17.0 Forth 29 10.7 Fifth 24 8.9 Family type Nuclear family Parents 184 67.9 Mother only 43 15.9 Father only 2 0.7 Extended family Parents, gra ndparents 25 9.2 Mother, grandparent 9 3.3 Father, gra ndparent 0 0.0 Other 8 3.0 Siblings Yes 176 64.9 No 95 35.1 Quantity of child care 11 hours or more 146 53.9 Less than 11 hours 125 46.1 Respondent Mother 254 93.7 Father 13 4.8 N.A. 4 1.5 Total 271 100.0 Copyright © 2012 SciRe s . 264 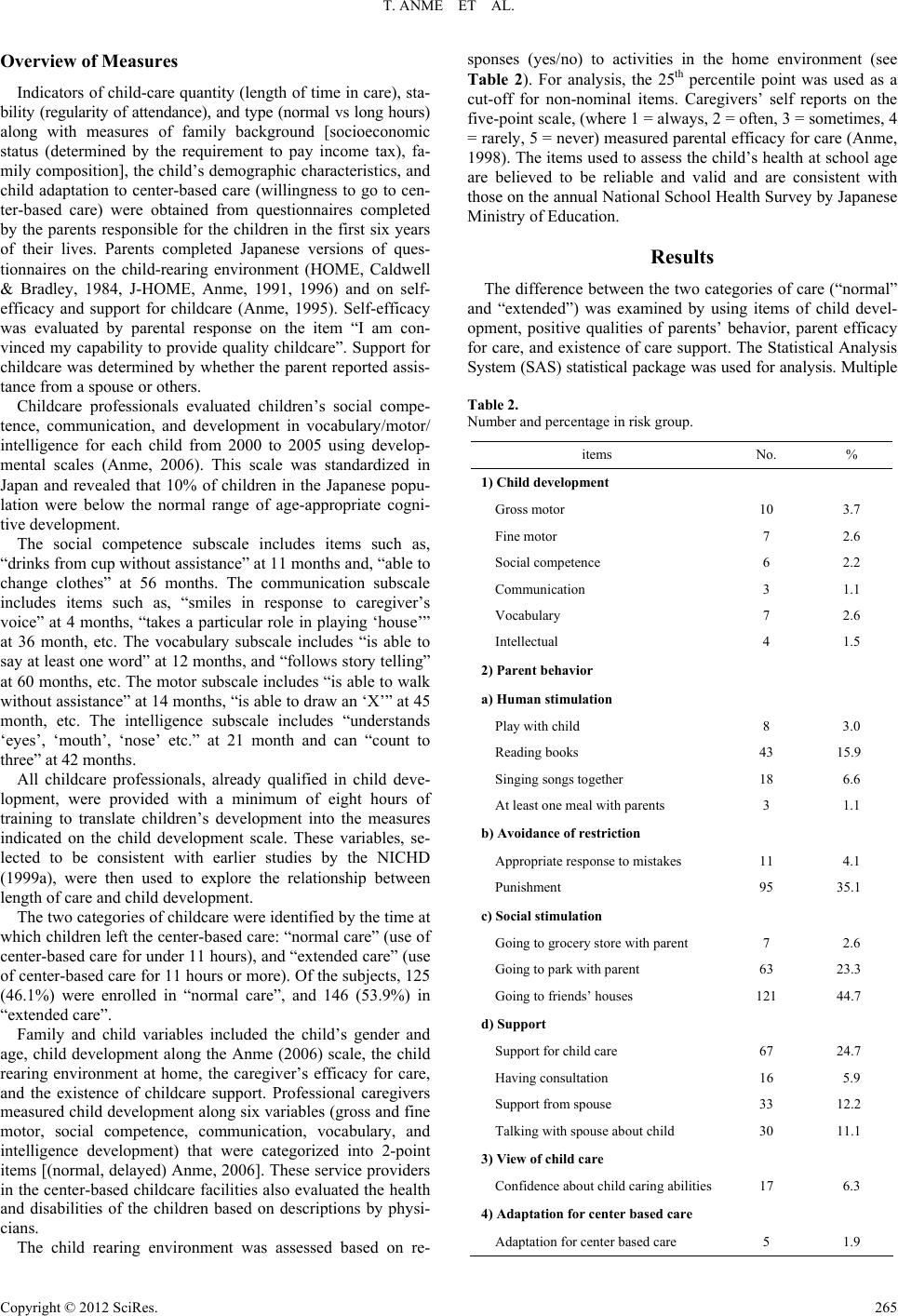 T. ANME ET AL. Overview of Measures Indicators of child-care quantity (length of time in care ), sta- bility (regularity of attendance), a nd type (normal vs long hours) along with measures of family background [socioeconomic status (determined by the requirement to pay income tax), fa- mily composition], the child’s demographic characteristics, and child adaptation to center-based care (willingness to go to cen- ter-based care) were obtained from questionnaires completed by the parents responsible for the children in the first six years of their lives. Parents completed Japanese versions of ques- tionnaires on the child-rearing environment (HOME, Caldwell & Bradley, 1984, J-HOME, Anme, 1991, 1996) and on self- efficacy and support for childcare (Anme, 1995). Self-efficacy was evaluated by parental response on the item “I am con- vinced my capability to provide quality childcare”. Support for childcare was determined by whether the parent reported assis- tance from a spouse or others. Childcare professionals evaluated children’s social compe- tence, communication, and development in vocabulary/motor/ intelligence for each child from 2000 to 2005 using develop- mental scales (Anme, 2006). This scale was standardized in Japan and revealed that 10% of children in the Japanese popu- lation were below the normal range of age-appropriate cogni- tive development. The social competence subscale includes items such as, “drinks from cup without assistance” at 11 months and, “able to change clothes” at 56 months. The communication subscale includes items such as, “smiles in response to caregiver’s voice” at 4 months, “takes a particular role in playing ‘house’” at 36 month, etc. The vocabulary subscale includes “is able to say at least one word” at 12 months, and “follows story telling” at 60 months, etc. The motor subscale includes “is able to walk without assistance” at 14 months, “is able to draw an ‘X’” at 45 month, etc. The intelligence subscale includes “understands ‘eyes’, ‘mouth’, ‘nose’ etc.” at 21 month and can “count to three” at 42 months. All childcare professionals, already qualified in child deve- lopment, were provided with a minimum of eight hours of training to translate children’s development into the measures indicated on the child development scale. These variables, se- lected to be consistent with earlier studies by the NICHD (1999a), were then used to explore the relationship between length of care and child development. The two categories of childcare were identified by the time at which children left the center-based care: “normal care” (use of center-based care for under 11 hours), and “extended care” (use of center-based care for 11 hours or more). Of the subjects, 125 (46.1%) were enrolled in “normal care”, and 146 (53.9%) in “extended care”. Family and child variables included the child’s gender and age, child development along the Anme (2006) scale, the child rearing environment at home, the caregiver’s efficacy for care, and the existence of childcare support. Professional caregivers measured child development along six variables (gross and fine motor, social competence, communication, vocabulary, and intelligence development) that were categorized into 2-point items [(normal, delayed) Anme, 2006]. These service providers in the center-based childcare facilities also evaluated the health and disabilities of the children based on descriptions by physi- cians. The child rearing environment was assessed based on re- sponses (yes/no) to activities in the home environment (see Table 2). For analysis, the 25th percentile point was used as a cut-off for non-nominal items. Caregivers’ self reports on the five-point scale, (where 1 = always, 2 = often, 3 = sometimes, 4 = rarely, 5 = never) measured parental efficacy for care (Anme, 1998). The items used to assess the child’s health at school age are believed to be reliable and valid and are consistent with those on the annual National School Health Survey by Japanese Ministry of Education. Results The difference between the two categories of care (“normal” and “extended”) was examined by using items of child devel- opment, positive qualities of parents’ behavior, parent efficacy for care, and existence of care support. The Statistical Analysis System (SAS) statistical package was used for analy sis. Multiple Table 2. Number and percentage in risk group. items No. % 1) Child development Gross motor 10 3.7 Fine motor 7 2.6 Social competence 6 2.2 Communication 3 1.1 Vocabulary 7 2.6 Intellectual 4 1.5 2) Parent be havior a) Human stimulation Play with child 8 3.0 Reading bo oks 43 15.9 Singing songs togeth er 18 6.6 At least one meal with parents 3 1.1 b) Avoidance of restriction Appropriate respons e to mistakes 11 4.1 Punishment 95 35.1 c) Social stimulation Going to groc ery store with p arent 7 2.6 Going to park with pare nt 63 23.3 Going to friends’ houses 121 44.7 d) Support Support for child care 67 24.7 Having con s ultation 16 5.9 Support from spouse 33 12.2 Talking with spouse a bo ut child 30 11.1 3) View of child care Confidenc e about chil d caring abil it ies 17 6.3 4) Adaptation for center based care Adaptation for center based care 5 1.9 Copyright © 2012 SciRe s . 265  T. ANME ET AL. regression analysis was used to predict child health symptoms at school age (yes or no) with independent variables such as types of care (“extended care” or else), positive qualities of parents’ behavior (13 items), parent efficacy for care, and exis- tence of care support, child development (delayed or normal) and child adaptation to center-based care (adapted or not) at toddler age. An odds ratio was calculated to clarify the magni- tude of effects. The odds ratio was calculated applying a multi- ple logistic analysis to estimate the strength of relations. All results were assessed significant at the p < .01 or p < .05 level, however, the variable “types of care” was not always selected as a related varia bl e in all analyses . Table 2 reports the number of risks in parent behavior. Table 3 shows correlations with the child’s health at school age. The maximum percentage is 17.0% for “easy to fatigue”, while the minimum percentage is 7.8% for poor physical strength. Table 4 reports the results of the Chi-square test between factors at the toddler age and the child’s health at school age. The delay of fine motor at the toddler age was significantly related to anxiety at school age. Interestingly, being the only child was related being easily fatigued at school age. Table 4 also presents the relationship between the care- giver’s factors expressed when the child was a toddler and the child’s health at school age. Not singing songs together in the early years was significa ntly related to poor physical strength at school age. Not going to the park with parents was related to headaches at school age. As indicated in Table 5, a multiple regression analysis, that input all factors and excluded the effects of gender and grade in school, was employed to explain children’s health at school age. Poor physical strength at school age was significantly related not playing with the child at the toddler age (odds ratio 3.23). Feelings of loneliness at school age was significantly related to not being adapted to center-based care at the toddler age (9.40). Discussion This is the first nation-wide study of center-based care that Table 3. Child’s health at school age. Item Yes (%) No (%) Feeling ove r whelmed 8.1 91.9 Anxious 11.4 88.6 Get irritated 15.1 84.9 Poor physical strength 7.8 92.2 Easy to fatig ue 17.0 83.0 Lonely 11.4 88.6 Displeasure and easy to get angry 14.0 86.0 Poor endura nce 13.7 86.3 Headache 10.7 89.3 Feel depressed 8.5 91.5 Want to attack someone 15.5 84.5 Lose interest in study 14.4 85.6 (n = 131) focuses on the effects of extended-hour care, including night care, and that assesses child health at school age based on the complex relations among factors, including the quality of par- ent behavior. Center-based extended-hour care through mid- night is unique in Japan, reflecting the increase in the number of parents who work late into the night. This investigation ex- plored the influence of extended-hour center-based care (over 11 hours of care per day, including night care), in comparison to normal care (11 hours or less). All night care centers in this study had passed governmental standards and attempted to ensure that the natural circadian rhythms for children, such as sleeping, eating, and playing, were well maintained. Several relatively recent large-scale, center-based childcare studies conducted outside Japan have documented relations between early and/or extensive childcare experience, noncom- pliance, and problem-behavior, even after controlling for selec- tion effects (Bates et al., 1994; Baydar & Brooks-Gunn, 1991; Belsky & Eggebeen, 1991; Borge & Melhuish, 1995; Park & Honig, 1991; Vandell & Corasaniti, 1990). Divergent results emerged from the current investigation, which found little evi- dence that the amount of time children spent in non-parental care in the first 2 or 3 years of life is, in and of itself, system- atically related to children’s self-control, compliance, or prob- lem behavior by the time they reach the school-age years. In light of prior studies and contemporary theory about the complex ecology of child development, the general absence of strong or consistent effects of the variable “type of care”, by itself, may not be surprising. The compensatory-process, and lost-resource perspectives outlined in the introduction led to the anticipation of findings that highlight interactions between quality and quantity of care and child development more than main effects of the length of center-based care. Although qua- lity was the most consistent predictor of child development, the amount of explained variance was modest, and standardized regression coefficients never exceeded .26 in the cumulative- experience analysis and/or .16 in the lagged-and-concurrent analysis. On the basis of analyses employed to identify selection-effect variables, several of the caregivers’ and family characteristics that distinguished between families that participated in this study, and those who did not, may be systematically related to childcare quality. Nevertheless, the high rate of return and the highly homogeneous nature of Japanese society may minimize these effects. That the home environment was more strongly related to child development and adaptation than was length of center-based care is consistent with results of prior examina- tions of the effects of childcare on infant-mother attachment (NICHD, 1998b) and child development (Langlois & Liben, 2003). The principal conclusion of this large-scale, multisite research project is that child rearing behavior by the caregiver may be more important in explaining children’s health at school age than whether parents routinely use the services of high quality center-based care facilities or the length of time children spend in these facilities. Items strongly related to child health at school age, such as “playing with child” in infancy, may serve as a proxy items for a number of factors at home, because they indicate the opportunity to engage in activities inside and out- side home, with other children, and in proximity of their care- givers. Literature does suggest, however, that center-based care ex- erts some influence upon children. Studies report that the qua- lity of care is the most consistnt child-care predictor, with e Copyright © 2012 SciRe s . 266 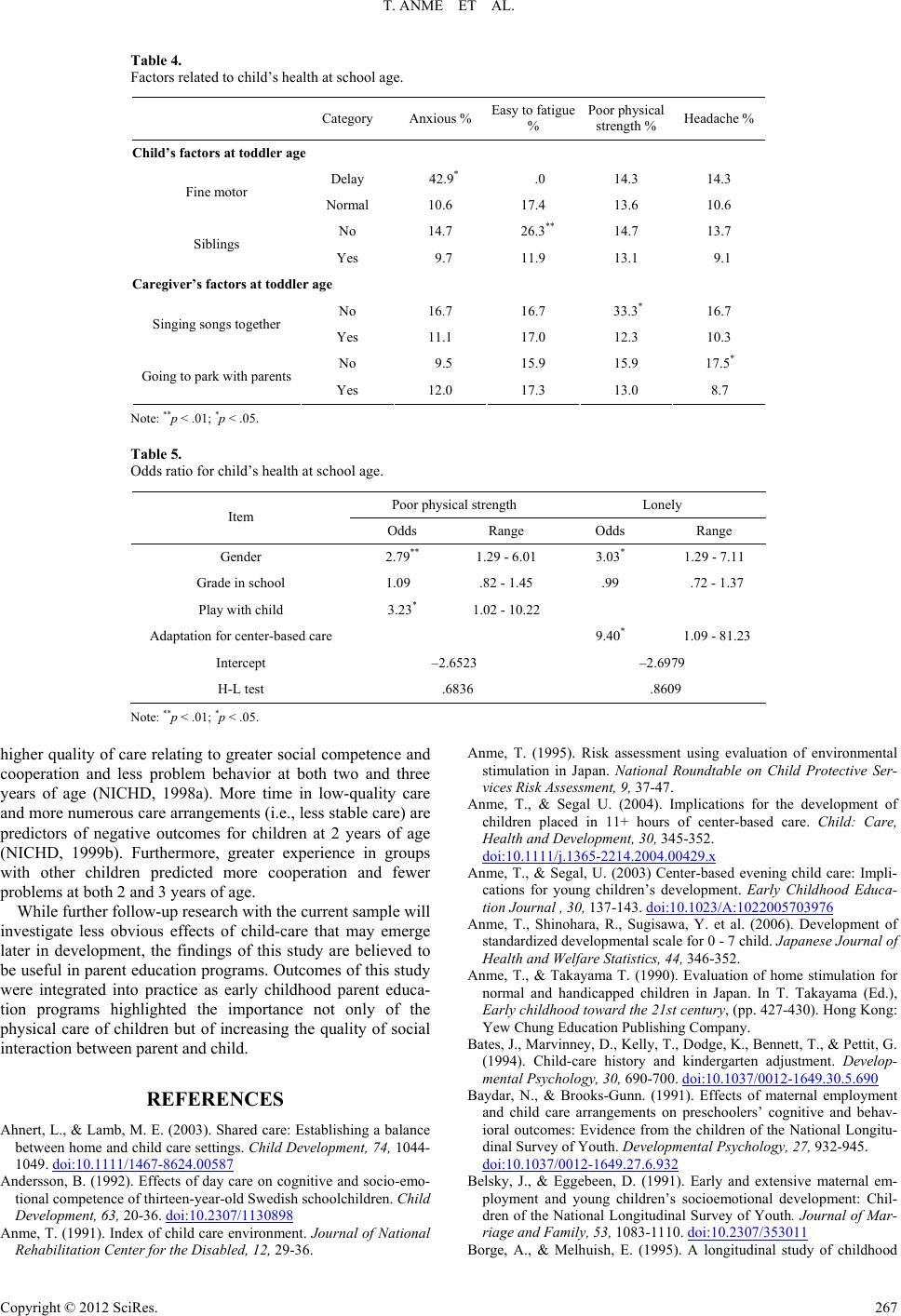 T. ANME ET AL. Copyright © 2012 SciRe s . 267 Table 4. Factors related to child’s health at sch ool age. Category Anxious % Easy to fatigue % Poor physical strength % Headache % Child’s factors at toddler age Delay 42.9* .0 14.3 14.3 Fine motor Normal 10.6 17.4 13.6 10.6 No 14.7 26.3** 14.7 13.7 Siblings Yes 9.7 11.9 13.1 9.1 Caregiver’s factors at toddler age No 16.7 16.7 33.3* 16.7 Singing songs together Yes 11.1 17.0 12.3 10.3 No 9.5 15.9 15.9 17.5* Going to park with parents Yes 12.0 17.3 13.0 8.7 Note: **p < .01; *p < .05. Table 5. Odds ratio for child’s health at scho ol age. Poor physical strength Lonely Item Odds Range Odds Range Gender 2.79** 1.29 - 6.01 3.03* 1.29 - 7.11 Grade in scho ol 1.09 .82 - 1.45 .99 .72 - 1.37 Play with child 3.23* 1.02 - 10.22 Adaptation for center-based care 9.40* 1.09 - 81.23 Intercept –2.6523 –2.6979 H-L test .6836 .8609 Note: **p < .01; *p < .05. higher quality of care relating to greater social competence and cooperation and less problem behavior at both two and three years of age (NICHD, 1998a). More time in low-quality care and more numerous care arrangements (i.e., less stable care) are predictors of negative outcomes for children at 2 years of age (NICHD, 1999b). Furthermore, greater experience in groups with other children predicted more cooperation and fewer problems at both 2 and 3 years of age. While further follow-up research with the current sample will investigate less obvious effects of child-care that may emerge later in development, the findings of this study are believed to be useful in parent education programs. Outcomes of this study were integrated into practice as early childhood parent educa- tion programs highlighted the importance not only of the physical care of children but of increasing the quality of social interaction between parent and child. REFERENCES Ahnert, L., & Lamb, M. E. (2003). Shared care: Establishing a balance between home and child care settings. Child Development, 74, 1044- 1049. doi:10.1111/1467-8624.00587 Andersson, B. (1992). Effects of day care on cognitive and socio-emo- tional competence of thirteen-year-old Swedish schoolchildren. Child Development, 63, 20-36. doi:10.2307/1130898 Anme, T. (1991). Index of child care environment. Journal of National Rehabilitation Center for the Disabled, 12, 29-36. Anme, T. (1995). Risk assessment using evaluation of environmental stimulation in Japan. National Roundtable on Child Protective Ser- vices Risk Assessment, 9, 37-47. Anme, T., & Segal U. (2004). Implications for the development of children placed in 11+ hours of center-based care. Child: Care, Health and Development, 30, 345-352. doi:10.1111/j.1365-2214.2004.00429.x Anme, T., & Segal, U. (2003) Center-based evening child care: Impli- cations for young children’s development. Early Childhood Educa- tion Journal , 30, 137-143. doi:10.1023/A:1022005703976 Anme, T., Shinohara, R., Sugisawa, Y. et al. (2006). Development of standardized developmental scale for 0 - 7 child. Japanese Journal of Health and Welfare Statistics, 44, 346-352. Anme, T., & Takayama T. (1990). Evaluation of home stimulation for normal and handicapped children in Japan. In T. Takayama (Ed.), Early childhood toward the 21st century, (pp. 427-430). Hong Kong: Yew Chung Education Publi s h ing Company. Bates, J., Marvinney, D., Kelly, T., Dodge, K., Bennett, T., & Pettit, G. (1994). Child-care history and kindergarten adjustment. Develop- mental Psychology, 30, 690-700. doi:10.1037/0012-1649.30.5.690 Baydar, N., & Brooks-Gunn. (1991). Effects of maternal employment and child care arrangements on preschoolers’ cognitive and behav- ioral outcomes: Evidence from the children of the National Longitu- dinal Survey of Youth. Developmental Psychology, 27, 932-945. doi:10.1037/0012-1649.27.6.932 Belsky, J., & Eggebeen, D. (1991). Early and extensive maternal em- ployment and young children’s socioemotional development: Chil- dren of the National Longitudinal Survey of Youth. Journal of Mar- riage and Family, 53, 1083-1110. doi:10.2307/353011 Borge, A., & Melhuish, E. (1995). A longitudinal study of childhood  T. ANME ET AL. behavior problems, maternal employment, and day care in rural Norwegian community. International Journal of Behavioral Devel- opment, 18, 23-42. Caldwell, B. M., & Bradley, R. H. (1984). Home observation for meas- urement of the environment. Little Rock: University of Arkansas at Little Rock. Crockenberg, S. C. (2002). Rescuing the baby from the bathwater: How gender and temperament (may) influence how child care affects child development. Child development, 74, 1034-1038. doi:10.1111/1467-8624.00585 Lamb, M. E. (1996). Effects of nonparental child care on child devel- opment: An update. Canadian Journal of Psychiatry, 41, 330-342. Langlois, J. H. & Liben, L. S. (2003). Child care research: An editorial perspective. Child Development, 74, 969-975. doi:10.1111/1467-8624.00581 Love, J. M., Harrison, L., Sagi-Schwartz, A., van Ijzendoorn, M. H., Rocc, C., & Ungerer, J. (2003). Child care quality matters: How con- clusions may vary with context. Child Development, 74, 1021-1033. doi:10.1111/1467-8624.00584 NICHD Early Child Care Research Network (1998a). The NICHD study of early child care. Psychiatric Times, 15, 71-72. NICHD Early Child Care Research Network (1998b). Relations be- tween family predictors and child outcomes: Are they weaker for children in child care? Developmental Psychology, 34, 1119-1128. doi:10.1037/0012-1649.34.5.1119 NICHD Early Child Care Research Network (1998c). Early child care and self-control, compliance and problem behavior at twenty-four and thirty-six months. Child Development, 69, 1145-1170. NICHD Early Child Care Research Network (1999a). Child outcomes when child care center classes meet recommended standards for quality. American Journal of Public Health, 89, 1072-1077. doi:10.2105/AJPH.89.7.1072 NICHD Early Child Care Research Network (1999b). Child care and mother-child interaction in the first three years of life. Developmen- tal Psychology, 35, 1399-1413. doi:10.1037/0012-1649.35.6.1399 NICHD Early Child Care Research Network (2001). Nonmaternal care and family factors in early development: An overview of the NICHD study of early child care. Journal of Applied Developmental Psy- chology, 22, 457-492. doi:10.1016/S0193-3973(01)00092-2 NICHD Early Child Care Research Network (2002a). Direct and indi- rect effects of child-care quality on young children’s development. Psychological Science, 13, 199-206. NICHD Early Child Care Research Network (2002b). The interaction of child care and family risk in relation to child development at 24 and 36 months. Applied Developmental Science, 6, 144-156. doi:10.1207/S1532480XADS0603_4 NICHD Early Child Care Research Network (2003). Does amount of time in child care predict socioemotional adjustment during the tran- sition to kindergarten: Child Development, 74, 976-1005. doi:10.1111/1467-8624.00582 Park, K., & Honig, A. (1991). Infant child care patterns and later teacher ratings of preschool behaviors. Early Child Development and Care, 68, 89-96. doi:10.1080/0300443910680108 Sacker, A., Schoon, I., & Bartley, M. (2002). Social inequality in edu- cation achievement and psychosocial adjustment throughout child- hood: Magnitude and mechanism. Social Science and Medicine, 55, 863-880. doi:10.1016/S0277-9536(01)00228-3 Salmela-Aro, K., & Schoon, I. (2005). Human development and well-being. Special issue. European Psychologist, 10, 259-263. doi:10.1027/1016-9040.10.4.259 Schoon, I. (2006). Risk and resilience: Adaptations to changing times. Cambridge: Cambridge University Press. doi:10.1017/CBO9780511490132 Schoon, I., Bynner, J., Joshi, H., Parsons, S., Wiggins, R. D. & Sacker, A. (2002). The influence of context, timing and duration of risk ex- periences for the passage from childhood to early adulthood. Child Development, 73, 1486-1504. doi:10.1111/1467-8624.00485 Vandell, D. L., & Corasaniti, M. A. (1990). Child care and the family: Complex contributors to child development. New directions for child development, 49, 23-37. doi:10.1002/cd.23219904904 Watamura, S. E., Donzella, B. Alwin, J., & Gunnar, M. R. (2003). Morning-to-afternoon increases in cortisol concentrations for infants and toddlers at child care: Age differences and behavioral correlates. Child Development, 74, 1006-1020. doi:10.1111/1467-8624.00583 Copyright © 2012 SciRe s . 268
|