T. NISHIZAKI ET AL.
20
tively non-fatal in comparison to hypertensive brainstem
hemorrhage [1,2]. Therefore, such patients often undergo
surgery. However, it is sometimes difficult to distinguish
patients with and without vascular malformation. Among
the present patients who survived, none of the repeated
MRI examinations revealed apparent vascular malforma-
tion during follow-up.
CT classification of pontine hemorrhage: CT classifi-
cation is an unequivocally useful tool for prognostication
in patients with brain hemorrhage. Massive and diffuse
pontine hemorrhages are likely to be more often fatal
than those that are subependymal or focal [8]. Russell et
al. subdivided pontine hematomas into three types on the
basis of CT findings: central, tegmentobasilar and dorso-
lateral tegmental [6]. Large hematomas resulting from
systemic hypertension generally occupy the central pons,
resulting in a fatal outcome, and involve the reticular
activating system, giving rise to abrupt coma with quad-
riplegia, a decerebrate posture, or pinpoint pupils. Other
types of hematoma include partial pontine hematomas
restricted to the lateral half of the pons with sparing of
the reticular system, and these can be either tegmento-
basilar or dorsolateral tegmental.
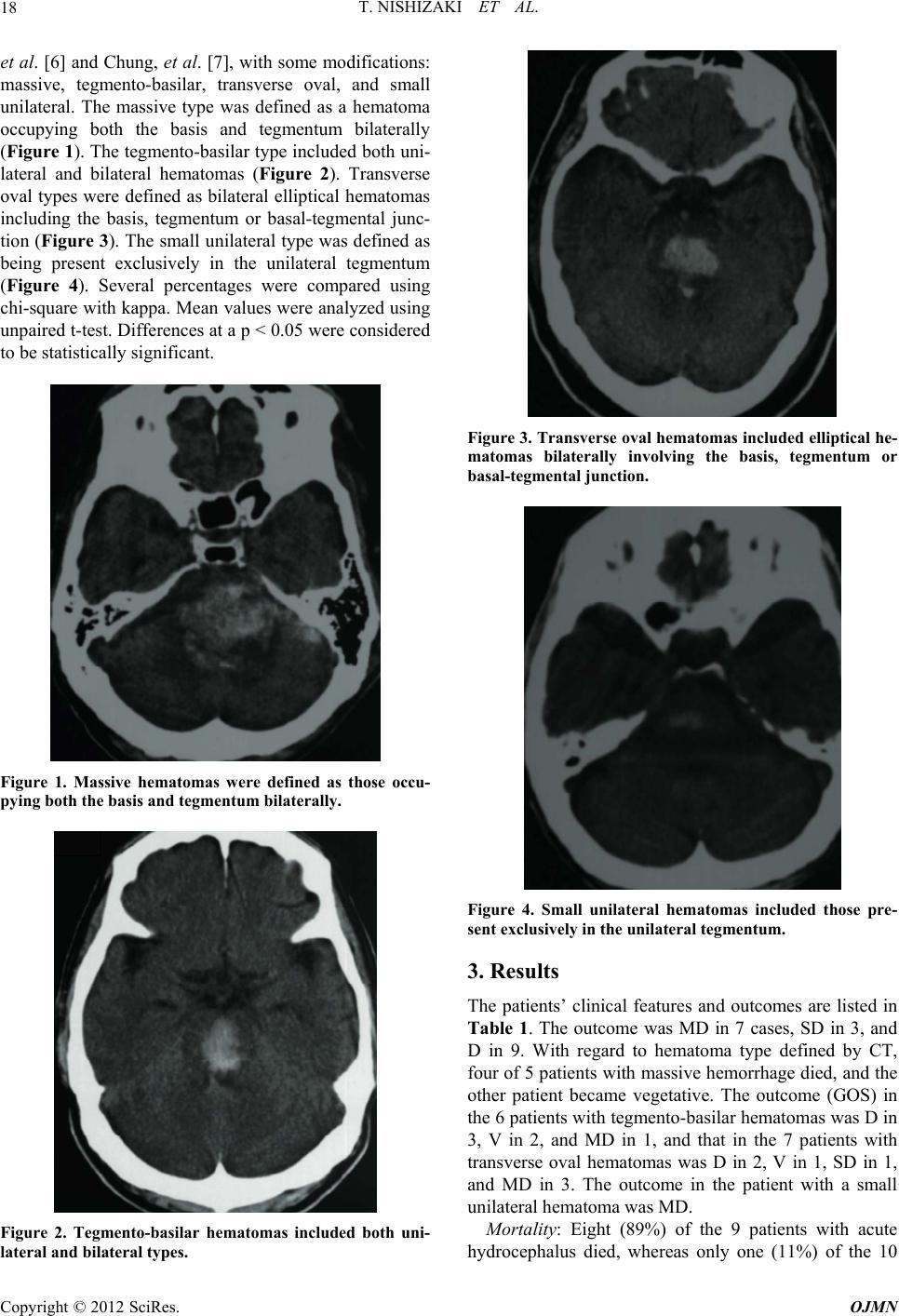
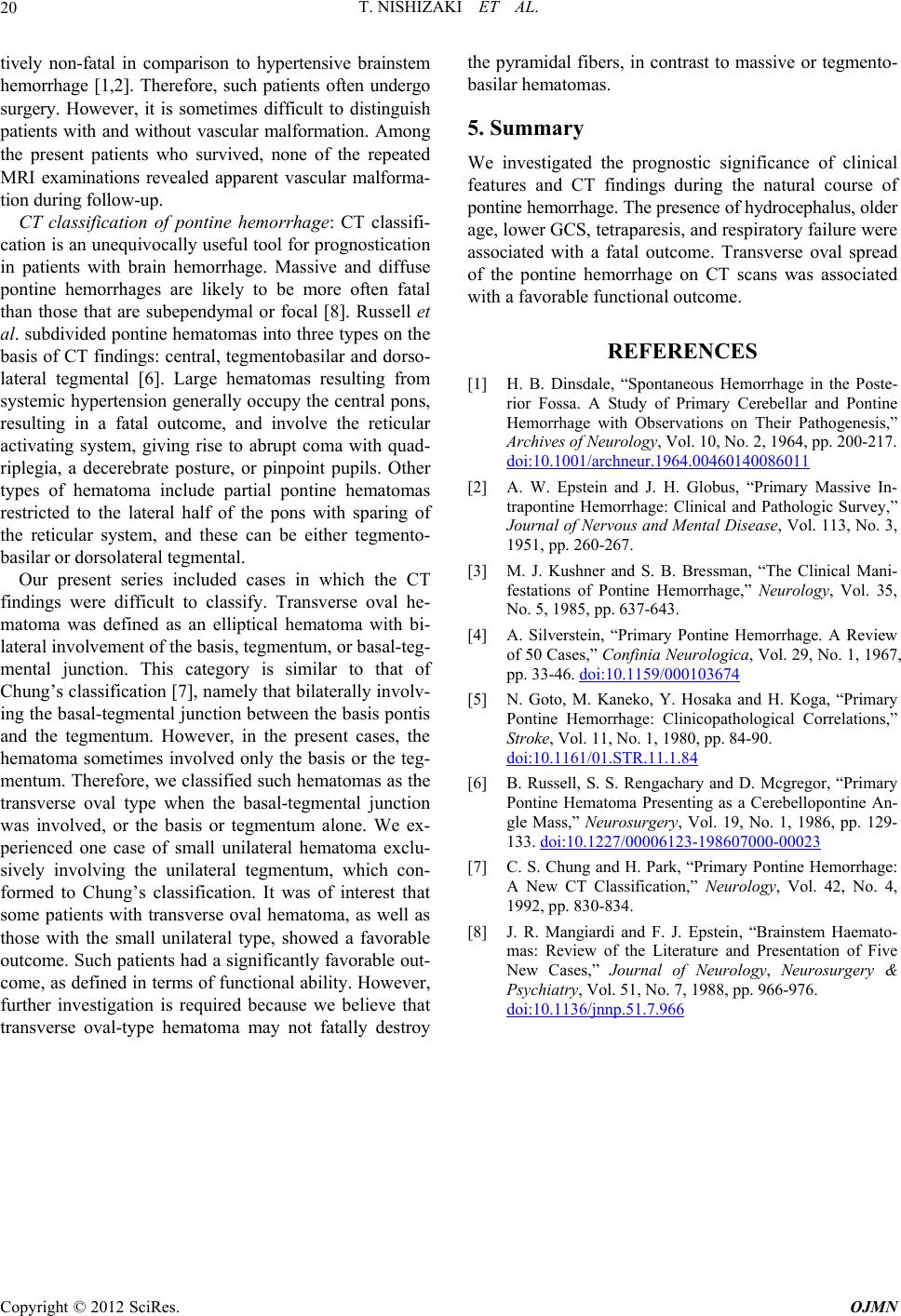
Our present series included cases in which the CT
findings were difficult to classify. Transverse oval he-
matoma was defined as an elliptical hematoma with bi-
lateral involvement of the basis, tegmentum, or basal-teg-
mental junction. This category is similar to that of
Chung’s classification [7], namely that bilaterally involv-
ing the basal-tegmental junction between the basis pontis
and the tegmentum. However, in the present cases, the
hematoma sometimes involved only the basis or the teg-
mentum. Therefore, we classified such hematomas as the
transverse oval type when the basal-tegmental junction
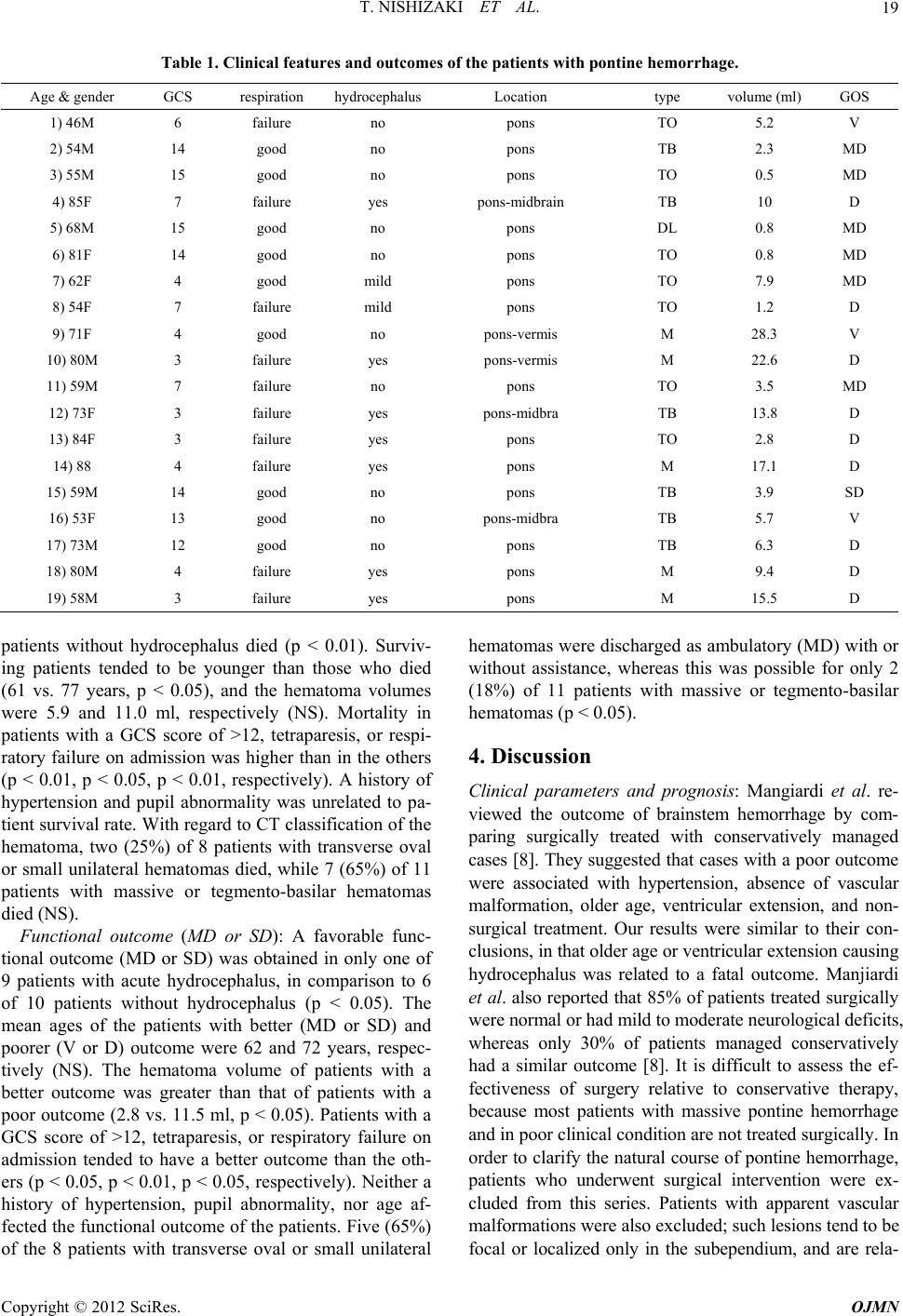
was involved, or the basis or tegmentum alone. We ex-
perienced one case of small unilateral hematoma exclu-
sively involving the unilateral tegmentum, which con-
formed to Chung’s classification. It was of interest that
some patients with transverse oval hematoma, as well as
those with the small unilateral type, showed a favorable
outcome. Such patients had a significantly favorable out-
come, as defined in terms of functional ability. However,
further investigation is required because we believe that
transverse oval-type hematoma may not fatally destroy
the pyramidal fibers, in contrast to massive or tegmento-
basilar hematomas.
5. Summary
We investigated the prognostic significance of clinical
features and CT findings during the natural course of
pontine hemorrhage. The presence of hydrocephalus, older
age, lower GCS, tetraparesis, and respiratory failure were
associated with a fatal outcome. Transverse oval spread
of the pontine hemorrhage on CT scans was associated
with a favorable functional outcome.
REFERENCES
[1] H. B. Dinsdale, “Spontaneous Hemorrhage in the Poste-
rior Fossa. A Study of Primary Cerebellar and Pontine
Hemorrhage with Observations on Their Pathogenesis,”
Archives of Neurology, Vol. 10, No. 2, 1964, pp. 200-217.
doi:10.1001/archneur.1964.00460140086011
[2] A. W. Epstein and J. H. Globus, “Primary Massive In-
trapontine Hemorrhage: Clinical and Pathologic Survey,”
Journal of Nervous and Mental Disease, Vol. 113, No. 3,
1951, pp. 260-267.
[3] M. J. Kushner and S. B. Bressman, “The Clinical Mani-
festations of Pontine Hemorrhage,” Neurology, Vol. 35,
No. 5, 1985, pp. 637-643.
[4] A. Silverstein, “Primary Pontine Hemorrhage. A Review
of 50 Cases,” Confinia Neurologica, Vol. 29, No. 1, 1967,
pp. 33-46. doi:10.1159/000103674
[5] N. Goto, M. Kaneko, Y. Hosaka and H. Koga, “Primary
Pontine Hemorrhage: Clinicopathological Correlations,”
Stroke, Vol. 11, No. 1, 1980, pp. 84-90.
doi:10.1161/01.STR.11.1.84
[6] B. Russell, S. S. Rengachary and D. Mcgregor, “Primary
Pontine Hematoma Presenting as a Cerebellopontine An-
gle Mass,” Neurosurgery, Vol. 19, No. 1, 1986, pp. 129-
133. doi:10.1227/00006123-198607000-00023
[7] C. S. Chung and H. Park, “Primary Pontine Hemorrhage:
A New CT Classification,” Neurology, Vol. 42, No. 4,
1992, pp. 830-834.
[8] J. R. Mangiardi and F. J. Epstein, “Brainstem Haemato-
mas: Review of the Literature and Presentation of Five
New Cases,” Journal of Neurology, Neurosurgery &
Psychiatry, Vol. 51, No. 7, 1988, pp. 966-976.
doi:10.1136/jnnp.51.7.966
Copyright © 2012 SciRes. OJMN