K. SIMON ET AL. 35
pendent marker for cardiovascular mortality [15]. On the
other hand, spirometry is in a large extent dependent on
the subject cooperation. As an illustration, as many as
11.5% of subjects are unable to perform correct forced
expiratory maneuvers, even in a young population with
little or no chronic lung disease [16]. Similarly, measur-
ing sRaw via plethysmography has advantages and dis-
advantages. The equipment is more sophisticated, more
expensive and the reproducibility is somewhat weaker
than that of FEV1, with e.g. a mean coefficient of varia-
tion of 9.3% in COPD patients in our laboratory [14]. On
the other hand, sRaw is more sensitive than FEV1 in a
large variety of clinical conditions. Studying the acute
effect of physiotherapy on lung function in patients with
copious sputum production, Cochrane et al. found a
greater change in sRaw than in FEV1 [17]. In patients
with heart-lung or bilateral lung transplantation, Bassiri
et al found that serial measurements of sRaw were more
useful than those of FEV1 for early detection of bron-
chiolitis obliterans syndrome [13].
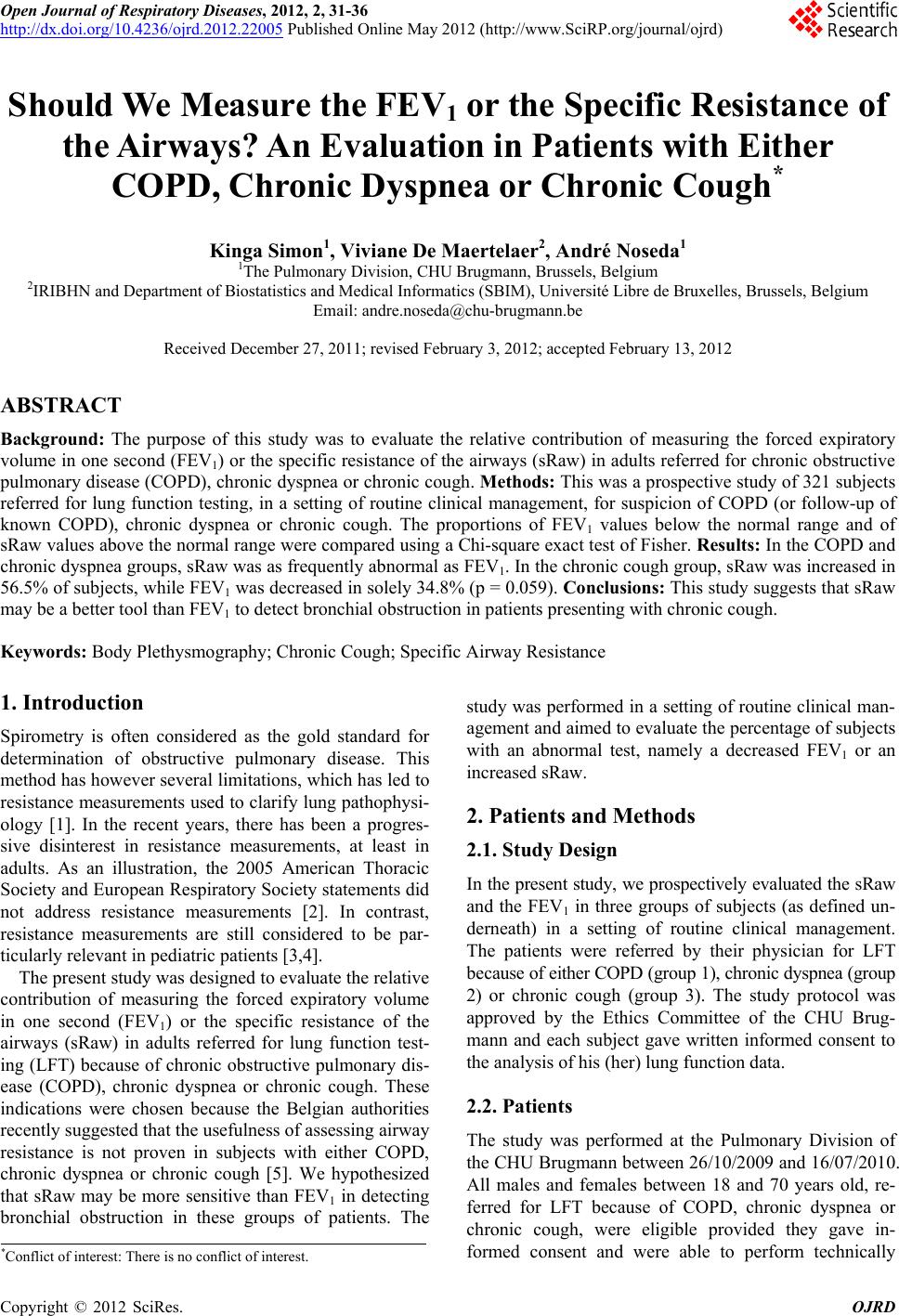
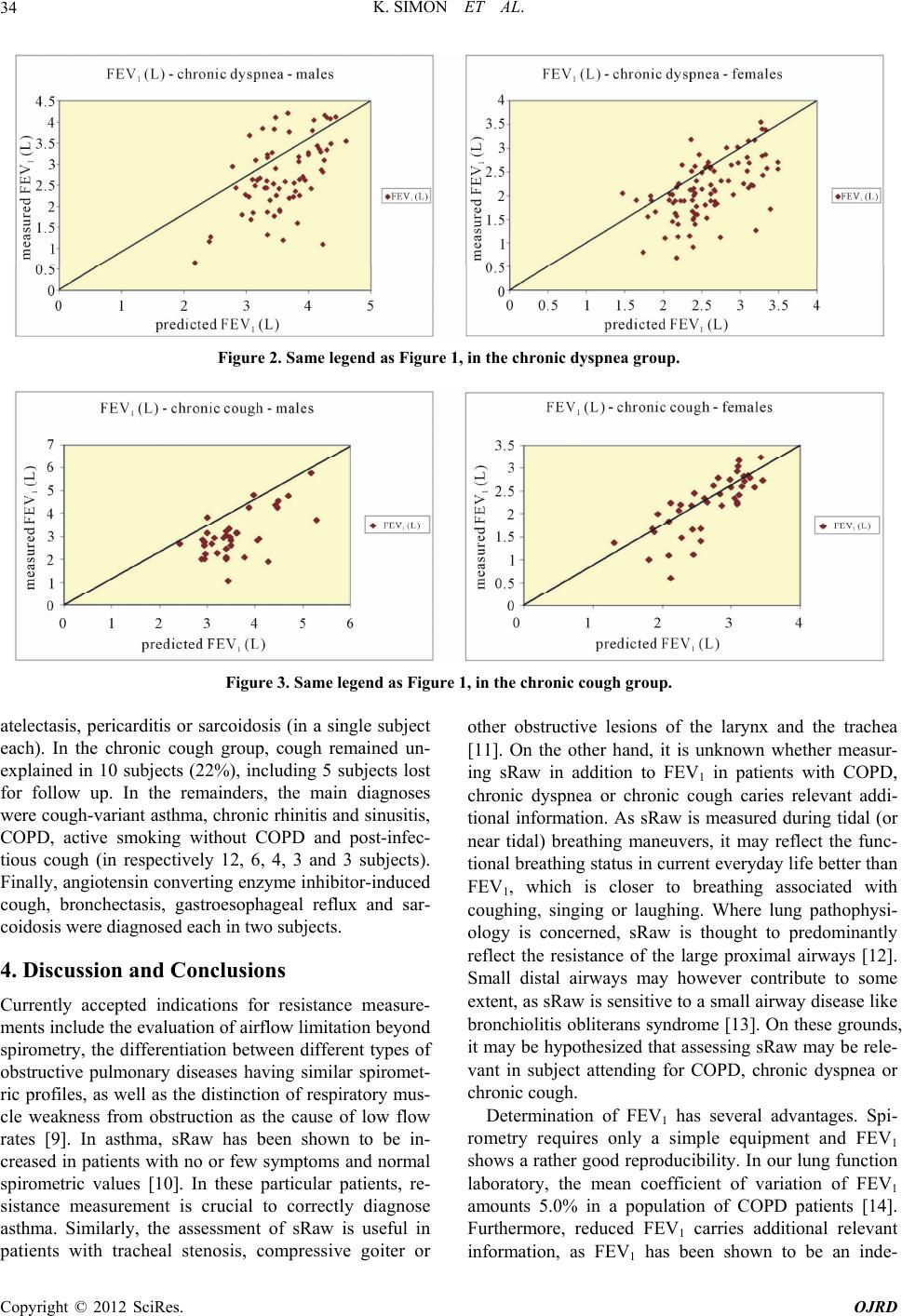
In the present study involving three groups of patients
with respectively COPD, chronic dyspnea and chronic
cough, we were able to show a larger proportion of sub-
jects with increased sRaw than that of subjects with de-
creased FEV1 only in chronic coughers. The difference
drew near statistical significance. On retrospective ex-
amination of medical charts, cough-variant asthma
emerged as the most frequent diagnosis retained to ex-
plain chronic cough. Cough-variant asthma is known to
be a frequent cause of chronic cough, particularly in non-
smokers. It may be either a precursor of typical asthma,
or persist lifelong as the sole symptom of asthma [18].
Definite diagnosis is usually based on both histamine or
metacholine inhalation testing and on resolution of cough
with anti-asthmatic therapy [19]. Studies on larger
groups of patients are needed to evaluate whether sRaw
may be a better tool than FEV1 to detect mild bronchial
obstruction in patients presenting with chronic cough.
5. Acknowledgements
The authors acknowledge Mrs F. Daimallah, Ch. Jacobs
and J. Roobaert for performing lung function testing, as
well as Mrs F. Martinez Vadillo for secretarial assis-
tance.
REFERENCES
[1] P. Calverley and N. Koulouris, “Flow Limitation and Dy-
namic Hyperinflation: Key Concepts in Modern Respiratory
Physiology,” European Respiratory Journal, Vol. 25, No.
1, 2005, pp. 186-199.
doi:10.1183/09031936.04.00113204
[2] American Thoracic Society, “Pulmonary Laboratory Man-
agement and Procedure Manual,” American Thoracic So-
ciety, New York, 2005.
[3] H. Bisgaard and K. G. Nielsen, “Plethysmographic Meas-
urements of Specific Airway Resistance in Young Chil-
dren,” Chest, Vol. 128, No. 1, 2005, 355-362.
doi:10.1378/chest.128.1.355
[4] J. Kirkby, S. Stanojevic, L. Welsh, S. Lum, M. Badier, C.
Beardsmore, A. Custovic, K. Nielsen, J. Paton and W.
Tomalak, “Reference Equations for Specific Airway Re-
sistance in Children: The Asthma UK Initiative,” Euro-
pean Respiratory Journal, Vol. 36, No. 3, 2010, pp. 622-
629. doi:10.1183/09031936.00135909
[5] A. Van den Bruel, J. Gailly, S. Devriese, F. Vritens and D.
Ramaekers, “Pulmonary Function Tests in Adults: Good
Clinical Practice,” Belgian Health Care Knowledge Cen-
tre, Brussels, 2007, KCE Reports 6.
[6] R. Peslin, A. Bohadana, B. Hannhart and P. Jardin, “Com-
parison of Various Methods for Reading Maximal Expi-
ratory Flow-Volume Curves,” American Review of Res-
piratory Disease, Vol. 119, 1979, pp. 271-277.
[7] Ph. H. Quanjer, A. Dalhuijsen and B. C. Van Zomeben,
“Summary Equations of Reference Values,” Bulletin Eu-
ropeen de Physiopathologie Respiratoire, Vol. 19, No. 5,
1983, pp. 45-51.
[8] A. M. Pelzer and M. L. Thomson, “Effect of Age, Sex,
Stature and Smoking Habits on Human Airway Conduc-
tance,” Journal of Applied Physiology, Vol. 21, No. 2,
1966, pp. 469-476.
[9] S. Blonshine and M. D. Goldman, “Optimizing Perform-
ance of Respiratory Airflow Resistance Measurements,”
Chest, Vol. 134, No. 6, 2008, pp. 1304-1309.
doi:10.1378/chest.06-2898
[10] D. A. Kaminsky, C. G. Irvin, D. A. Gurka, D. C. Feldsien,
E. M. Wagner, M. C. Liu and S. E. Wenzel, “Peripheral
Airways Responsiveness to Cool, Dry Air in Normal and
Asthmatic Individuals,” American Journal of Respiratory
and Critical Care Medicine, Vol. 152, No. 6, 1995, pp.
1784-1790.
[11] R. D. Miller and R. E. Hyatt, “Obstructing Lesions of the
Larynx and Trachea: Clinical and Physiologic Character-
istics,” Mayo Clinic Proceedings, Vol. 44, 1969, pp. 145-
161.
[12] P. T. Macklem and T. Mead, “Resistance of Central and
Peripheral Airways Measured by Retrograde Catheter,”
Journal of Applied Physiology, Vol. 22, No. 3, 1967, pp.
395-401.
[13] A. G. Bassiri, R. E. Girgis, R. L. Doyle and J. Theodore,
“Detection of Small Airway Dysfunction Using Specific
Airway Conductance,” Chest Vol. 111, No. 6, 1997, pp.
1533-1535. doi:10.1378/chest.111.6.1533
[14] A. Noseda, J. Schmerber, T. Prigogine and J. C. Yernault,
“Perceived Effect on Shortness of Breath of an Acute In-
halation of Saline or Terbutaline: Variability and Sensi-
tivity of a Visual Analogue Scale in Patients with Asthma
or COPD,” European Respiratory Journal, Vol. 5, 1992,
pp. 1043-1053.
[15] D. D. Sin, L. Wu and S. F. Man, “The Relationship be-
tween Reduced Lung Function and Cardiovascular Mor-
tality: A Population-Based Study and a Systematic Re-
Copyright © 2012 SciRes. OJRD