Four Years of Altering Neurological Symptoms:
A Rare Case of a Massive Left Ventricular Thrombus in the Absence of any Symptomatic Cardiac Disease
14
to his symptoms, few weeks later he experienced a pro-
nounced dysmetria and severe loss of spatial orientation.
Finally, diminished cognitive power and word finding
problems brought him to seek for another neurological
consultation.
Multiple ischemic lesions typical of embolic character
and of different age were detected on a subsequent cra-
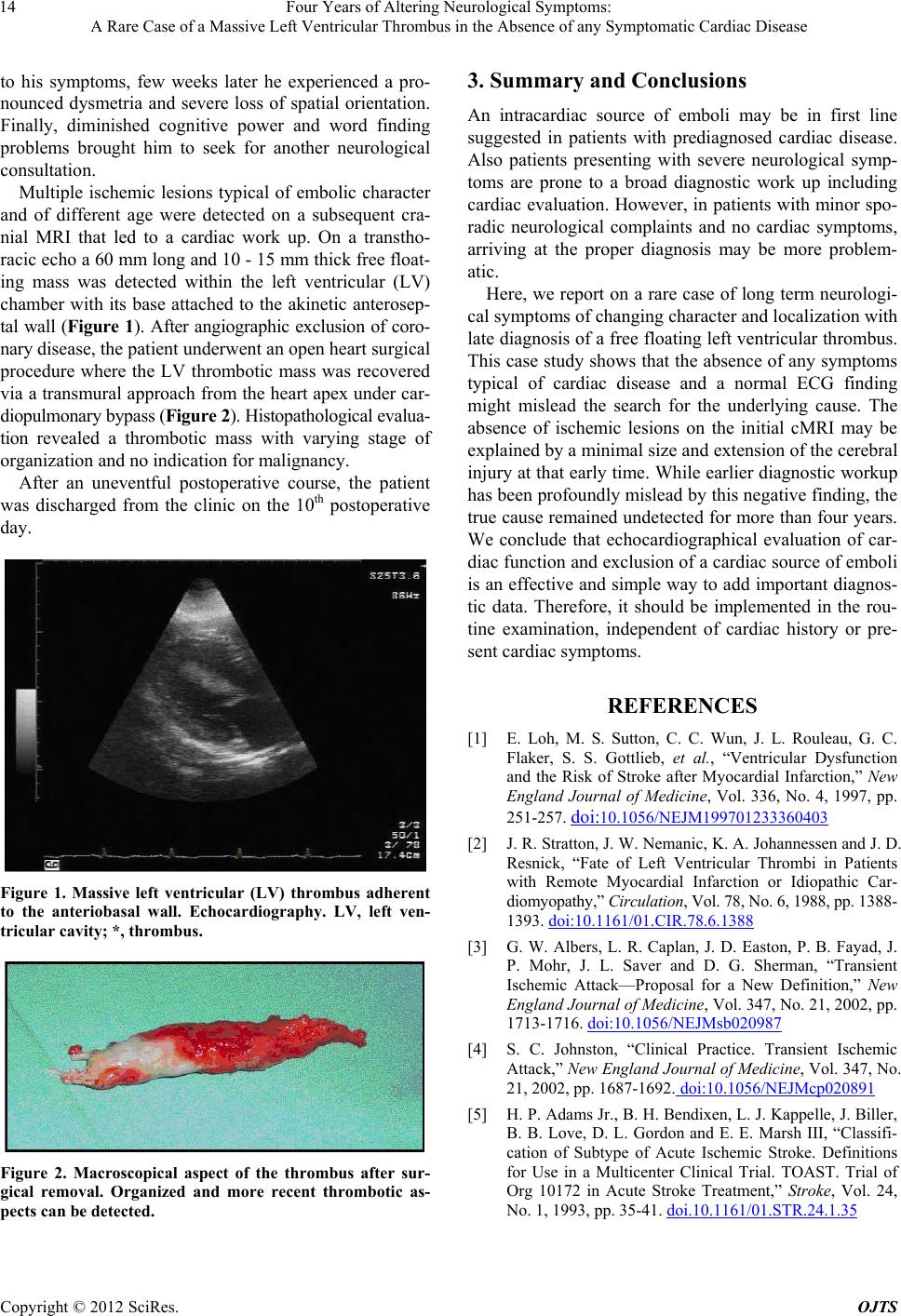
nial MRI that led to a cardiac work up. On a transtho-
racic echo a 60 mm long and 10 - 15 mm thick free float-
ing mass was detected within the left ventricular (LV)
chamber with its base attached to the akinetic anterosep-
tal wall (Figure 1). After angiographic exclusion of coro-
nary disease, the patient underwent an open heart surgical
procedure where the LV thrombotic mass was recovered
via a transmural approach from the heart apex under car-
diopulmonary bypass (Figure 2). Hist opat hologi cal evalua-
tion revealed a thrombotic mass with varying stage of
organization and no indication for malignancy.
After an uneventful postoperative course, the patient
was discharged from the clinic on the 10th postoperative
day.
Figure 1. Massive left ventricular (LV) thrombus adherent
to the anteriobasal wall. Echocardiography. LV, left ven-
tricular cavity; *, thrombus.
Figure 2. Macroscopical aspect of the thrombus after sur-
gical removal. Organized and more recent thrombotic as-
pects can be detected.
3. Summary and Conclusions
An intracardiac source of emboli may be in first line
suggested in patients with prediagnosed cardiac disease.
Also patients presenting with severe neurological symp-
toms are prone to a broad diagnostic work up including
cardiac evaluation. However, in patients with minor spo-
radic neurological complaints and no cardiac symptoms,
arriving at the proper diagnosis may be more problem-
atic.
Here, we report on a rare case of long term neurologi-
cal symptoms of changing character and localization with
late diagnosis of a free floating left ventricular thrombus.
This case study shows that the absen ce of any symptoms
typical of cardiac disease and a normal ECG finding
might mislead the search for the underlying cause. The
absence of ischemic lesions on the initial cMRI may be
explained by a minimal size and extension of the cerebral
injury at that early time. While earlier diag nostic workup
has been profoundly mislead by this negative finding, the
true cause remained undetected for more than four years.
We conclude that echocardiographical evaluation of car-
diac function and exclusion of a cardiac source of emboli
is an effective and simple way to add important diagnos-
tic data. Therefore, it should be implemented in the rou-
tine examination, independent of cardiac history or pre-
sent cardiac symptoms.
REFERENCES
[1] E. Loh, M. S. Sutton, C. C. Wun, J. L. Rouleau, G. C.
Flaker, S. S. Gottlieb, et al., “Ventricular Dysfunction
and the Risk of Stroke after Myocardial Infarction,” New
England Journal of Medicine, Vol. 336, No. 4, 1997, pp.
251-257. doi:10.1056/NEJM199701233360403
[2] J. R. Stratton, J. W. Nema nic, K. A. Johannessen and J. D.
Resnick, “Fate of Left Ventricular Thrombi in Patients
with Remote Myocardial Infarction or Idiopathic Car-
diomyopathy,” Circulation, Vol. 78, No. 6, 1988, pp. 1388-
1393. doi:10.1161/01.CIR.78.6.1388
[3] G. W. Albers, L. R. Caplan, J. D. Easton, P. B. Fayad, J.
P. Mohr, J. L. Saver and D. G. Sherman, “Transient
Ischemic Attack—Proposal for a New Definition,” New
England Journal of Medicine, Vol. 347, No. 21, 2002, pp.
1713-1716. doi:10.1056/NEJMsb020987
[4] S. C. Johnston, “Clinical Practice. Transient Ischemic
Attack,” New England Journal of Medicine, Vol. 347, No.
21, 2002, pp. 1687-1692. doi:10.1056/NEJMcp020891
[5] H. P. Adams Jr., B. H. Bendixen, L. J. Kappelle, J. Bille r,
B. B. Love, D. L. Gordon and E. E. Marsh III, “Classifi-
cation of Subtype of Acute Ischemic Stroke. Definitions
for Use in a Multicenter Clinical Trial. TOAST. Trial of
Org 10172 in Acute Stroke Treatment,” Stroke, Vol. 24,
No. 1, 1993, pp. 35-41. doi.10.1161/01.STR.24.1.35
Copyright © 2012 SciRes. OJTS
