Open Journal of Ophthalmology, 2012, 2, 5-7
http://dx.doi.org/10.4236/ojoph.2012.21002 Published Online February 2012 (http://www.SciRP.org/journal/ojoph) 5
Another Proliferative Diabetic Retinopathy? A Case
Report of Retinal Cavernous Haemangioma Treated
with Intravitreal Bevacizumab, Initially Labelled as
Persistent Proliferative Diabetic Retinopathy
Myrto Tsagkataki1*, Ahmad Khalil1, Ahmed Kamal1
1Ophthalmology Department, Aintree University Hospitals, Liverpool, United Kingdom.
Email: *m.tsagkataki@gmail.com
Received November 19th, 2011; revised December 24th, 2011; accepted January 25th, 2012.
ABSTRACT
We present a case of Retinal Cavernous Haemangioma treated with Intravitreal Bevacizumab, which was initially la-
belled as persistent proliferative diabetic retinopathy with multiple episodes of v itreous haemorrhage. These lesions can
be confused with new retinal vessels in diabetics and if correctly diagnosed unnecessary photocoagulation can be
avoided. Our patient received a course of three intravitreal Bevacizumab injections (1.25 mg/0.05 ml) in order to stop
the leakage from the retinal cavernous haemangioma lesions and prevent another episode of vitreous haemorrhage. No
intraoperative or postoperative complications were seen. Twenty-two months following treatment there was no recur-
rence of vitreous haemorrhage.
Keywords: Retinal Cavernous Haemangioma; Intravitreal Bevacizumab; Persistent Proliferative Diabetic Retinopathy;
Vitreous Haemorrhage
1. Introduction
We would like to report a case of Retinal Cavernous
Haemangioma treated with Intravitreal Bevacizumab,
which was initially diagnosed as persistent proliferative
diabetic retinopathy with multiple episodes of vitreous
haemorrhage.
2. Case
A 59 year-old insulin dependent diabetic male was re-
ferred from another ophthalmic unit with a diagnosis of
persistent retinal neovascularisation in the left eye, de-
spite repeat sessions of laser photocoagulation. He had a
history of multiple mild to moderate self-limiting vitre-
ous haemorrhages in the past which settled without any
surgical intervention. Previous medical history apart
from diabetes mellitus was insignificant. On examination
Best-Corrected Visual Acuity (BCVA) was logMAR
0.00 OD and 0.18 OS. Anterior segment examination
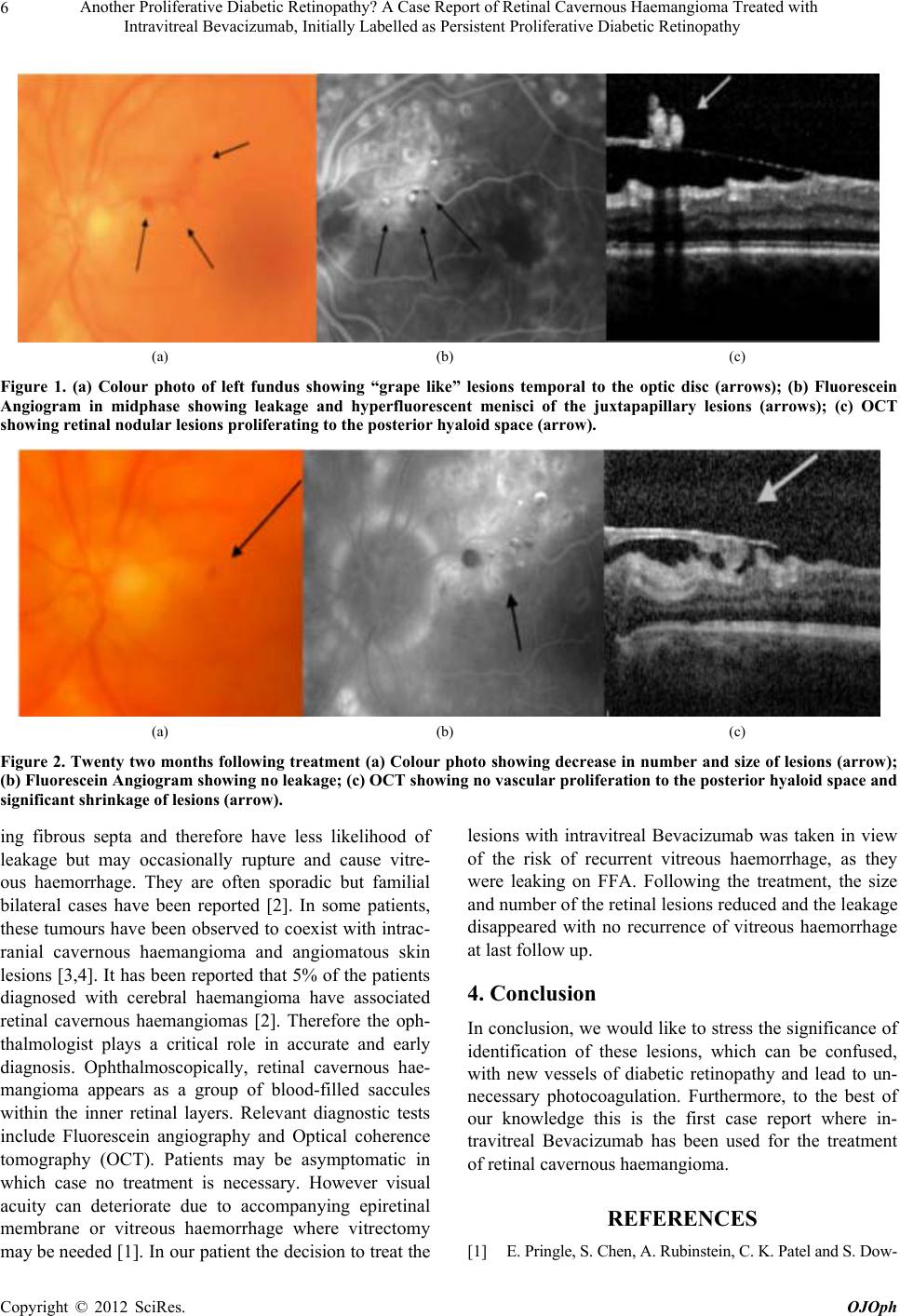
was unremarkable. Fundus exa mination showed a cluster
of abnormal vessels in the juxtapapillary region of the
temporal retina (Figure 1(a)). Fluorescein Angiography
(FFA) showed saccular lesions with slow filling in the
early phase and late hyperfluorescence with typical fluid
levels within the saccules (Figure 1(b)).Optical Coher-
ence Tomography (OCT) showed a bunch of “gr a pe-l i ke” ,
nodular retinal lesions proliferating to the posterior hya-
loid space (Figure 1(c)). The working diagnosis was
Retinal Cavernous Haemangioma. MRI brain and orbit
was then performed which didn’t show any abnormalities.
A decision was made to treat the patient with a view to
shrink these lesions and prevent a recurrence of vitreous
haemorrhage. The patient received monthly intravitreal
injections of Bevacizumab (1.25 mg/0.05 ml) for three
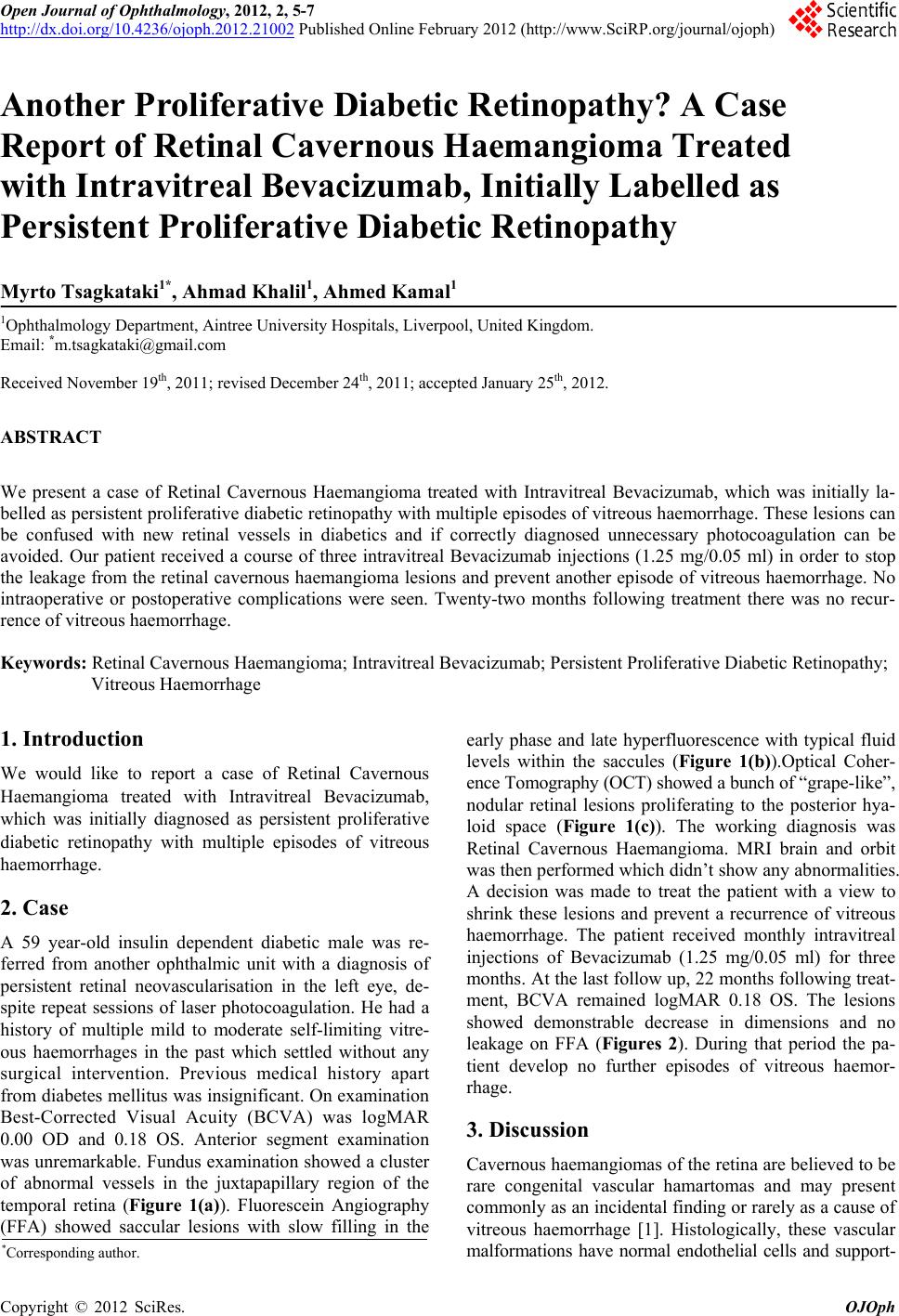
months. At the last follow up, 22 months following treat-
ment, BCVA remained logMAR 0.18 OS. The lesions
showed demonstrable decrease in dimensions and no
leakage on FFA (Figures 2). During that period the pa-
tient develop no further episodes of vitreous haemor-
rhage.
3. Discussion
Cavernous haemangiomas of the retina are believed to be
rare congenital vascular hamartomas and may present
commonly as an incidental finding or rarely as a cause of
vitreous haemorrhage [1]. Histologically, these vascular
alformations have normal endothelial cells and support- m
*Corresponding a uthor.
Copyright © 2012 SciRes. OJOph