 Psychology 2012. Vol.3, No.1, 70-77 Published Online January 2012 in SciRes (http://www.SciRP.org/journal/psych) http://dx.doi.org/10.4236/psych.2012.31012 Copyright © 2012 SciRes. 70 Sensory Processing Difficulties and Interpersonal Relationships in Adults: An Exploratory Study Nili Ben-Avi1, Moshe Almagor1, Batya Engel-Yeger2 1Department of Psychology, Haifa University, Haifa, Israel 2Occupational Therapy Department, Faculty of Social Welfare and Health Sciences, University of Haifa, Haifa, Israel Email: niliofir@gmail.com Received September 21st, 2011; revised November 4th, 2011; accepted December 8th, 2011 The purpose of this study was to investigate the association between sensory processing difficulties (SPD) which refers to detection, modulation and response to sensory input and interpersonal relationships. 139 students participated in the study and completed two self report questionnaires: The Adolescent/Adult Sensory Profile measuring sensory processing abilities as expressed in daily living and the Hebrew ver- sion of the MMPI-2. The results demonstrated strong associations between different patterns of SPD and a wide range of symptomathology, including anxiety, somatization, distress, and demoralization, difficu- lties in social interactions, family, work and therapeutic relationships. The findings of this study indicate that extreme sensory processing patterns are strongly related to distress and psychological difficulties. Therefore, it is recommended that clinical therapists relate to sensory processing as part of their dynamic conceptualization of patients’ difficulties. This also emphasizes the significance of interdisciplinary treat- ment that takes sensory processing into consideration in order to create an intervention program that con- siders the person’s specific sensory needs and their relationship with personality. Keywords: Sensory Processing; MMPI-2; Interpersonal Relationships; Sensory Processing Difficulties; Demoralization Introduction Individual’s personality interacts with the way one integrates sensory and experienced events (Bender & Schilser in Chutroo, 2007). The association between individual’s sensory processing capacities and various clinical features has been examined in only few studies, focusing mainly on depression, anxiety and emotional regulation (e.g., Kinnealey & Fuiek, 1999; Liss, Ti- mmel, Baxley, & Killingsworth, 2005). The present study aims to elaborate this association, particularly regarding interper- sonal relationships in typically healthy individuals. Sensory Processing Sensory processing relates to the way one detects, regulates, interprets and responds to sensory stimuli (Dunn, 2001). Senso- ry processing includes physiological and behavioral compo- nents: The physiological aspect of the process relates to stru- ctural changes or the functioning of the nervous system (Kandel, 1991). The behavioral aspect relates to the individual’s capacity to regulate reactions to stimuli adaptively to the environmental requirements (Royeen & Lane, 1991). Typical sensory proce- ssing enables adaptive and organized reactions to environmen- tal demands, while atypical patterns of sensory processing may negatively influence the functioning of the individual in every- day life (Tal-Saban et al., 2002; Dunn, 2001). It is estimated that 15% of the typical population experiences different levels of atypical sensory processing patterns (Simeonsson et al., 2003). Atypical sensory processing or SPD may be expressed by hypersensitivity or hyposensitivity to sensory stimuli; this de- pends on neurological threshold for sensory stimuli. A low neu- rological threshold indicates that the individual requires low in- tensity stimuli for the individual to react, while individuals with a high neurological threshold need high intensity stimuli or take longer to react to the same stimuli (Dunn, 2001). Wilbarger and Wilbarger (1991) defined hypersensitivity as the tendency to have a negative reaction to a sensory input that is commonly considered harmless, as for example, hypersensitivity to odors or noises in a room; tactile sensitivity to specific fabrics. On the other hand, hyposensitivity is defined as a decreased sensitivity to stimuli in the environment. A common consequence is inat- tention to injuries, behavior such as excessive touching and increased activity (Wilbarger & Wilbarger, 1991). Cermak (1998) described hypersensitivity and hyposensitivity as two extremes on the same continuum and not as separate phenomena, as the contention was until then. Thus, hypersensi- tivity in one sensory system may coexist with hyposensitivity in another system (Royeen, 1989). Dunn’s Model for Sensory Processing Dunn’s (1997) model of sensory processing comprises two axes of sensory processing: the neurological threshold of the individual (high or low) and his/her behavioral response. According to Dunn’s (1997) model, for each of the neurolo- gical thresholds, the behavioral response strategy can be active or passive. An active behavioral response is expressed by ac- tions that aim to cope with the neurological threshold. A pas- sive behavioral response is characterized by a lack of effort to reduce or increase the stimulation, even if the stimulus does not match the neurological threshold.  N. BEN-AVI ET AL. The interactions between the threshold and behavioral re- sponse axes form four orthogonal quadrants: 1) Sensation Avoi- ding—which represents low neurological thresholds and an active response strategy. This quadrant characterizes active avoidance of sensory stimuli in order to reduce uncomfortable experience; 2) Sensory Seekers-high neurological thresholds and an active response strategy. Persons in the quadrant will try to meet their neurological threshold actively seek high intensity stimuli in order to actively increase the strength of the response; 3) Sensory Sensitivity-low neurological threshold and a passive behavioral response. Individuals in this quadrant will not act actively to stop or reduce the level of sensory threshold while experiencing discomfort. 4) Low Registration-passive response and high neurological threshold, these persons will respond to sensory stimuli either slowly or not at all to. The Sensory pro- cessing patterns are likely to have an impact on the individual’s psychological functioning. The Sensory Processing Patterns an d I nt e r p e rs o n a l Relationshi ps among Adults Dunn’s Model for Sensory Processing Sensory Seeking Patter n: High Neurological Threshold and Active Behavioral Response This behavior can lead to social rejection due to the lack of the physical boundaries and a dangerous behavior that is con- sidered by others as irresponsible, impatient and lacking respect for others. According to Miller, Anzalone, Lane, Cermak, and Osten (2007), people with a “sensory seeking” profile demonstrate activities meant to increase sensory experience, such as an increased mo- tor behavior, forming contact with objects and people (like bu- mping into objects) and seeking strong stimuli such as spicy food, strong noises and stimulating visual. In social context, these behaviors represent over affection and an attempt to initi- ate interpersonal contact in a non-informative way, seeking to boost their sensory experiences so that the sensory input crosses their reaction threshold This behavior may result in social re- jection due to lack of physical boundaries and dangerous be- havior that may be considered by others as irresponsible, impa- tient and disrespectful. MMPI-2 is one of the most commonly used personality tests in mental health to assist in assessing psychopathology and pe- rsonality structure and is composed of a large number of scales providing a comprehensive description of the person. Correla- tions between sensation seeking and several MMPI-2 scales ha- ve already been reported. A positive correlation was found, for both men and women, between sensation seeking and scale 9 (Ma), which is associated with impulsivity and hyperactivity (McKinley & Hathaway, 1944; Zuckerman & Bone, 1972; Zuc- kerman & Link, 1968). This correlation was explained by the high activity level and the need for varied and intense stimuli (Zuckerman & Link, 1968). Other studies found an association between sensation seeking and low scores on scale 0 (Si, Social extroversion-Introversion) low scores measures behavior characteristic of extroversion (Dunn, 2001; Eysenck, 1967; Sutker, Archer, & Allain, 1978; Zuckerman & Bone, 1972; Zuckerman & Link, 1968). Low Registry Pattern: High Neurological Threshold and Passive Behavioral Response Common characteristic of people with a “low registry” sen- sory processing profile is the tendency to react easily or not to react at all, to strong and even damaging stimuli. Children are described as quiet, obedient, as having a low level of arousal and as having trouble learning about their environment (Royeen & Lane, 1991). Persons characterized by this pattern are typi- cally lacking in reaction to sensory stimuli, which may be per- ceived as indifference, sluggishness and lack of motivation or interest in the world in general and in initiating relationships in particular. Lack of response doesn’t stem from lack of motiva- tion but rather from an absence of sensory reaction, leading to inability to recognize possibilities for action. Common examples include lack of reaction to falls, injuries or abnormal tempera- ture (Miller, Anzalone, Lane, Cermak, & Osten, 2007) inability to recognize and express emotions and lack of sense of humor (Dunn, 1997). Sensory Avoidance Pattern: Low Neurological Threshold and Active Behavioral Response Individuals who fit the “sensory avoidance” quadrant are cha- racterized by an active attempt to avoid sensory stimuli due to intense sensory reaction to every sensory stimulus. These reac- tions produce tension, anxiety and nervousness, and problems in initiating relationships. These individuals are likely to have aggressive and negative reactions to intense, overwhelming and invasive sensory stimuli (Miller, Anzalone, Lane, Cermak, & Osten, 2007). The negative reactions can be expressed by se- clusion, social withdrawal and avoidance of outdoor activities such as traveling by automobile or plane. Sensory Sensitivity Patte r n: Low Neurological Threshold and Passive Behavioral Response Individuals with the “sensory sensitivity” pattern experience intense sensory reactions to every sensory stimulus, and there- fore they also tend to be characterized by feelings of tension, anxiety and nervousness, and problems in initiating relation- ships. These individuals can have aggressive and negative reac- tions to sensory stimuli that they experienced as intense, over- whelming and invasive (Miller, Anzalone, Lane, Cermak, & Osten, 2007). Sensory Proce s si n g and Psychol o g i ca l C haracterist i c s SPD are related to behavioral and adjustment problems of children, particularly those associated with emotional regula- tion, depression and anxiety. Sensory hypersensitivity has been found to be related to lack of sleep, hyper-emotionality, exa- ggerated defense mechanisms and incapacity to complete new assignments (Royeen & Lane, 1991; Wilbarger & Wilbarger, 1991).Children (or their parents) are the main population that appeals for treatment, therefore the measures for SPD was first developed for children. Even though research on sensory processing has been condu- cted mostly on children, and we have reason to believe that Chil- dren suffer from these difficulties more than adults, who learn and adapted their life to live with the situation, there is some evidence that adults with SPD also experience higher levels of anxiety, depression and adjustment problems, (Kinnealey & Fuiek, 1999). Liss, Timmel, Baxley, and Killingsworth’s (2005) found significant connections between sensory hypersensitivity and psychological distress, anxiety and depression. Considering the fact that sensory processing profiles remain constant over time, further research is necessary to determine the relationship between sensory processing and psychological aspects among Copyright © 2012 SciRes 71  N. BEN-AVI ET AL. adults as well. The current research aims to contribute to the en- deavor. Goal of Cu rrent Study The present study aims to explore and expand our knowledge on the association between sensory sensitivity and social skills among adults. Specifically, the purpose of this study is to ex- plore the relationships between Dunn’s four sensory processing patterns and the quality of interpersonal and social relationships among typical adults. The study is unique in that it focuses on this aspect among typical healthy adults; the study uses a com- bination of measures which were not previously applied in this population: the MMPI-2 and the Adolescent/Adult Sensory Pro- file Questionnaire (AASP). The main hypothesis was that adult participants with SPD will show different symptoms related to interpersonal relationships compared to participants with typi- cal sensory processing. Method Participants and Design One-hundred thirty nine undergraduate students participated in the study for credit and were recruited by computerized ex- periment registration system of the department of Psychology at University of Haifa. Credit points were offered to each student willing to participate in the experiment. Thirteen participants did not match the inclusion criteria and were omitted from the statistical analysis (subjects with nervous system injuries, aller- gies or taking medications which affect the central nervous system). The MMPI-2 of three additional subjects was invalid (according to the MMPI-2 criteria ); and were also omitted from the statistical analysis. Thus, the statistical analysis was con- ducted on 123 subjects: 36 men and 86 women. All subjects spoke native Hebrew, all reported general overall good health, did not report any kind of chronic disease and did not take medications that affect the nervous system. The age of the sub- jects ranged between 19 and 33 (M = 23.85, SD = 2.44), with a significant gender difference: the men were significantly older (M = 24.72, SD = 2.73) than the women (M = 23.48, SD = 2.05), [t(121) = 2.77, p < .01]. Measures Background and Physical Condition Questionnaire In this brief questionnaire, subjects were asked to report their gender and age and answer several questions regarding their health. The Adolescent/Adult Sensory Profile Questionnaire (ASP) is a self-report measure developed by Dunn and Brown (2002) as a trait measure of sensory processing patterns and effects on daily life behavior. The AASP consists of 60 items (on a 5-po- int Likert scale) regarding how he or she generally responds to different sensations. Fifteen items represent each of the four quadrants, or sensory profile types. The sensory processing ca- tegories are taste, smell, movement, sight, touch, hearing and activity level (proprioception). These categories are distributed throughout each of the 15 items included in each quadrant. The current study found adequate reliabilities. Each of the four qua- drants shows high Cronbach’s coefficient of internal consis- tency. The questionnaire was translated to Hebrew by Parush, En- gel-Yeger and Ben-Sason (2006). The current study uses the norms developed by Dunn and Brown (2002) in the United States for the same age groups, since the norms in Israel have not yet been developed. In Dunn & Brown’s normative sample, an adequate freque- ncy of responses matched the criteria for three of the four sen- sory profiles: sensory sensitivity, sensory avoiding and low re- gistry. Therefore, comparisons can be made between the per- sonality characteristics of those respondents who had a normal or a low rate and those who had a higher than average score on each of these three sensory profiles (see Table 1). The Minnesota Multiphasic Personality Inventory (MMPI-2) The MMPI-2 (Butcher, Dahlstrom, Graham, Tellegan, & Kae- mmer, 1989) provides extensive clinical, symptomatic, person- ality and interpersonal evaluation of the individual’s mental state. The version used here is the Hebrew translation (Almagor, 2005). The MMPI-2 has high reliability and validity (Almagor, 2005 ; Graham, 2005; Greene, 2010) . Procedure The research procedure was approved by the Haifa Univer- sity ethics committee for experiments on humans (Approval nu- mber 080/80). All subjects signed an informed consent that de- scribed the study, procedures to ensure anonymity and confi- dentiality, and provision of psychological help if requested. Su- bjects were told they can quit the experiment at any point. Students were told that the experiment deals with personality structure and sensory experiences in everyday life, and that it involves only filling questionnaires. The questionnaires were administered in a balanced order: Half completed the computerized MMPI-2 first, and then filled out the sensory profile questionnaire. The other half completed the experiment in the reverse order. In order to control for order of administration, MANOVA procedures were employed were conducted using Hotelling’s Trace criterion. No significant di- fferences were found between the two groups. The administra- tion was done in groups. Each group included 8 - 15 participants. The entire experiment lasted for an hour and a half. Results In order to control for the gender effect, two MANOVA pro- cedures were employed using Hotelling’s Trace criterion. No significant differences were found between men and women in the weighted variable of the sensory profile scores [F(4, 118) = .66, n.s]. However, there were significant differences between men and women for the weighted MMPI-2 scales variable [F(36, 86) = 4.45, p < .001].Therefore, gender was controlled during data a- nalyses. There was no significant between gender and each one of the sensory types for weighted MMPI-2 scale scores. In or- der to control for the age effect, Pearson correlations between the subjects’ age and the scores in the MMPI-2 scales and the Table 1. Frequency of respondents by intensity of sensory profile type (N = 123). Intensity Sensory sensitivity Sensory avoiding Sensory seeking Low registry Low 5 6 18 9 Normal88 87 95 84 High 30 30 10 30 Copyright © 2012 SciRes. 72 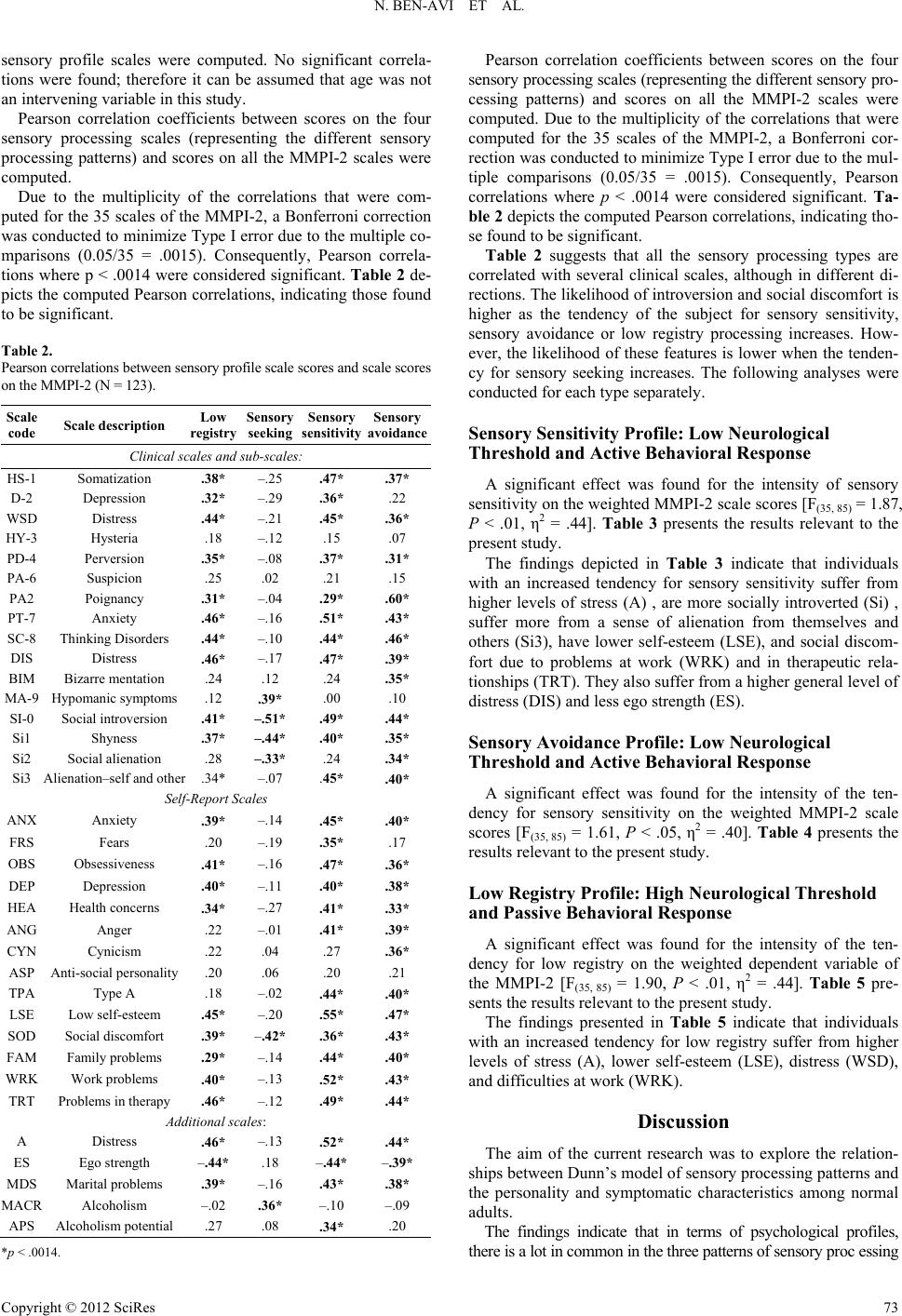 N. BEN-AVI ET AL. sensory profile scales were computed. No significant correla- tions were found; therefore it can be assumed that age was not an intervening variable in this study. Pearson correlation coefficients between scores on the four sensory processing scales (representing the different sensory processing patterns) and scores on all the MMPI-2 scales were computed. Due to the multiplicity of the correlations that were com- puted for the 35 scales of the MMPI-2, a Bonferroni correction was conducted to minimize Type I error due to the multiple co- mparisons (0.05/35 = .0015). Consequently, Pearson correla- tions where p < .0014 were considered significant. Table 2 de- picts the computed Pearson correlations, indicating those found to be significant. Table 2. Pearson correlations between sensory profile scale scores and scale scores on the MMPI-2 (N = 123). Scale code Scale descr i ption Low registry Sensory seeking Sensory sensitivity Sensory avoidance Clinical scales and sub-scales: HS-1 Somatization .38* –.25 .47* .37* D-2 Depression .32* –.29 .36* .22 WSD Distress –.21 .44* .45* .36* HY-3 Hysteria .18 –.12 .15 .07 PD-4 Perversion .35* –.08 .37* .31* PA-6 Suspicion .25 .02 .21 .15 PA2 Poignancy .31* –.04 .29* .60* PT-7 Anxiety .46* –.16 .51* .43* SC-8 Thinking Disorders .44* –.10 .44* .46* DIS Distress .46* –.17 .47* .39* BIM Bizarre mentation .24 .12 .24 .35* MA-9 Hypomanic symptoms .12 .39* .00 .10 SI-0 Social introversion .41* –.51* .49* .44* Si1 Shyness .37* –.44* .40* .35* Si2 Social alienation .28 –.33* .24 .34* Si3 Alienation–self and other .34* –.07 .45* .40* Self-Report Scales ANX Anxiety .39* –.14 .45* .40* FRS Fears .20 –.19 .35* .17 OBS Obsessiveness .41* –.16 .47* .36* DEP Depression .40* –.11 .40* .38* HEA Health concerns .34* –.27 .41* .33* ANG Anger .22 –.01 .41* .39* CYN Cynicism .22 .04 .27 .36* ASP Anti-social personality .20 .06 .20 .21 TPA Type A .18 –.02 .44* .40* LSE Low self-esteem .45* –.20 .55* .47* SOD Social discomfort .39* –.42* .36* .43* FAM Family problems .29* –.14 .44* .40* WRK Work problems .40* –.13 .52* .43* TRT Problems in therapy .46* –.12 .49* .44* Additional scales: A Distress .46* –.13 .52* .44* ES Ego strength –.44*.18 –.44* –.39* MDS Marital problems .39* –.16 .43* .38* MAC Alcoholism –.02 .36* –.10 –.09 APS Alcoholism potential .27 .08 .34* .20 *p < .0014. Pearson correlation coefficients between scores on the four sensory processing scales (representing the different sensory pro- cessing patterns) and scores on all the MMPI-2 scales were computed. Due to the multiplicity of the correlations that were computed for the 35 scales of the MMPI-2, a Bonferroni cor- rection was conducted to minimize Type I error due to the mul- tiple comparisons (0.05/35 = .0015). Consequently, Pearson correlations where p < .0014 were considered significant. Ta- ble 2 depicts the computed Pearson correlations, indicating tho- se found to be significant. Table 2 suggests that all the sensory processing types are correlated with several clinical scales, although in different di- rections. The likelihood of introversion and social discomfort is higher as the tendency of the subject for sensory sensitivity, sensory avoidance or low registry processing increases. How- ever, the likelihood of these features is lower when the tenden- cy for sensory seeking increases. The following analyses were conducted for each type separately. Sensory Sensitivit y Pr ofi l e: L ow Neurological Threshold and Active Behavioral Response A significant effect was found for the intensity of sensory sensitivity on the weighted MMPI-2 scale scores [F(35, 85) = 1.87, P < .01, η2 = .44]. Table 3 presents the results relevant to the present study. The findings depicted in Table 3 indicate that individuals with an increased tendency for sensory sensitivity suffer from higher levels of stress (A) , are more socially introverted (Si) , suffer more from a sense of alienation from themselves and others (Si3), have lower self-esteem (LSE), and social discom- fort due to problems at work (WRK) and in therapeutic rela- tionships (TRT). They also suffer from a higher general level of distress (DIS) and less ego strength (ES). Sensory Avoidance Profile: Low Neurological Threshold and Active Behavioral Response A significant effect was found for the intensity of the ten- dency for sensory sensitivity on the weighted MMPI-2 scale scores [F(35, 85) = 1.61, P < .05, η2 = .40]. Table 4 presents the results relevant to the present study. Low Registry Profi le : Hig h Neurological T hreshol d and Passive Behavioral Response A significant effect was found for the intensity of the ten- dency for low registry on the weighted dependent variable of the MMPI-2 [F(35, 85) = 1.90, P < .01, η2 = .44]. Table 5 pre- sents the results relevant to the present study. The findings presented in Table 5 indicate that individuals with an increased tendency for low registry suffer from higher levels of stress (A), lower self-esteem (LSE), distress (WSD), and difficulties at work (WRK). Discussion The aim of the current research was to explore the relation- ships between Dunn’s model of sensory processing patterns and the personality and symptomatic characteristics among normal adults. The findings indicate that in terms of psychological profiles, there is a lot in common in the three patterns of sensory proc essing Copyright © 2012 SciRes 73 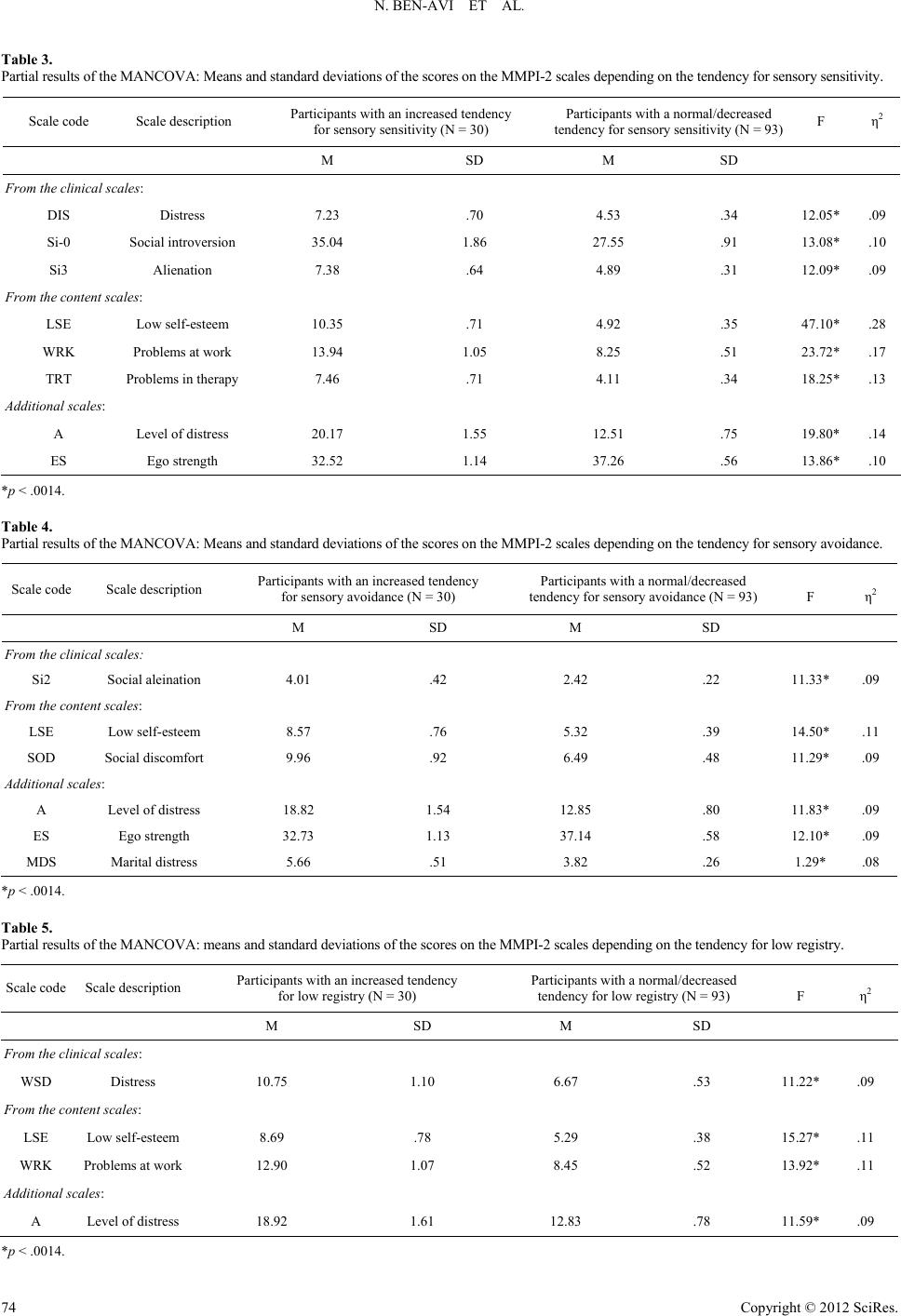 N. BEN-AVI ET AL. Copyright © 2012 SciRes. 74 Table 3. Partial results of the MANCOVA: Means and standard deviations of the scores on the MMPI-2 scales depending on the tendency for sensory sensitivity. Scale code Scale description Participants with an increased tendency for sensory sensitivity (N = 30) Participants with a normal/decreased tendency for sensory sensitivity (N = 93) F η2 M SD M SD From the clinic a l scales: DIS Distress 7.23 .70 4.53 .34 12.05*.09 Si-0 Social introversion 35.04 1.86 27.55 .91 13.08*.10 Si3 Alienation 7.38 .64 4.89 .31 12.09*.09 From the content scales: LSE Low self-esteem 10.35 .71 4.92 .35 47.10*.28 WRK Problems at work 13.94 1.05 8.25 .51 23.72*.17 TRT Problems in therapy 7.46 .71 4.11 .34 18.25*.13 Additional scales: A Level of distress 20.17 1.55 12.51 .75 19.80*.14 ES Ego strength 32.52 1.14 37.26 .56 13.86*.10 *p < .0014. Table 4. Partial results of the MANCOVA: Means and standard deviations of the scores on the MMPI-2 scales depending on the tendency for sensory avoidance. Scale code Scale description Participants with an increased tendency for sensory avoidance (N = 30) Participants with a normal/decreased tendency for sensory avoidance (N = 93) F η2 M SD M SD From the clinica l s cales: Si2 Social aleination 4.01 .42 2.42 .22 11.33*.09 From the content scales: LSE Low self-esteem 8.57 .76 5.32 .39 14.50*.11 SOD Social discomfort 9.96 .92 6.49 .48 11.29*.09 Additional scales: A Level of distress 18.82 1.54 12.85 .80 11.83*.09 ES Ego strength 32.73 1.13 37.14 .58 12.10*.09 MDS Marital distress 5.66 .51 3.82 .26 1.29* .08 *p < .0014. Table 5. Partial results of the MANCOVA: means and standard deviations of the scores on the MMPI-2 scales depending on the tendency for low registry. Scale code Scale description Participants with an increased tendency for low registry (N = 30) Participants with a normal/decreased tendency for low registry (N = 93) F η2 M SD M SD From the clinic a l scales: WSD Distress 10.75 1.10 6.67 .53 11.22*.09 From the content scales: LSE Low self-esteem 8.69 .78 5.29 .38 15.27*.11 WRK Problems at work 12.90 1.07 8.45 .52 13.92*.11 Additional scales: A Level of distress 18.92 1.61 12.83 .78 11.59*.09 *p < .0014.  N. BEN-AVI ET AL. “sensory sensitivity”, “sensory avoidance” and “low registra- tion”. The stronger the tendency of the subject for one or more of this patterns, the higher is the likelihood they will report more anxiety, somatization, distress characteristics, interperso- nal difficulties, lack of ego strength, thought distortions and poignancy. The only variables that had significant correlations with all sensory profiles were scales measuring aspects of Introversion; Social Introversion (SI), Shyness (SI1, a subscale of SI), and Social Discomfort (SOD). These three variables correlated po- sitively with Sensory Sensitivity, Sensory Avoidance, and Low Registration Sensory types, but negatively with Sensory Seek- ing type. The current study indicates that compared to individuals with a normal neurological threshold, individuals with atypical sen- sory pattern demonstrated lower self-esteem, more social dis- comfort, more distress and less ego strength. Furthermore, it was found that those with a low neurological threshold and a passive behavioral response report more social introversion, distress and problems at work. In contrast, parti- cipants with a low neurological threshold and an active beha- vioral response showed a higher score on the alienation from self and other scale and more problems in the family. The finding of the current study that individuals with sensory sensitivity are characterized by a higher level of social introver- sion, shyness, and social discomfort supports earlier studies which found similar associations (Aron & Aron, 1997; Aron, Aron, & Davies, 2005). Sensory Sensitivit y Pr ofi l e: L ow Neurological Threshold and Active Behavioral Response Since high scorers on Sensory Sensitivity experience intense sensory reactions to sensory stimuli, they are likely to control their physical environment by accommodating it to their special tendencies and needs. As opposed to the physical environment, the social environment is more difficult, sometimes even im- possible to control. This may explain their feelings of tension, anxiety and nervousness, and their problems in initiating social relationships. Sensory Avoidance Profile: Low Neurological Threshold and Active Behavioral Response The findings of the current study suggest interpersonal diffi- culties characterizing individuals with a Sensory Avoidance ty- pe as opposed to those with a Sensory Sensitivity type. These variables include social alienation, social isolation, interperso- nal difficulties and family problems and crises. High Neurological Threshold The findings of the current study indicate that a high neuro- logical threshold may be related to either a tendency for intro- version or extroversion, depending on the response strategy (ac- tive or passive). Previous studies found a relationship between sensory hypersensitivity and social introversion and shyness (Aron & Aron, 1997 ; Aron, Aron, & Davies, 2005). The current study suggests that social introversion is strongly related to sen- sory processing, when. high levels of sensory processing are re- lated to high levels of introversion or extroversion. These find- ings have a theoretical significance given the little research on the subject of high neurological thresholds. Low Registry Type: High Neurological Threshold and Passive Behavioral Response Individuals with low registry are characterized by a lack of response to sensory stimuli, and they may appear as indifferent and lacking interest in the world. There is very little empirical research on this type of processing. The tendency for social introversion that includes social wi- thdrawal, shyness and lack of self esteem in social situations in- creased as the tendency for low registry processing increased. The findings of the current study suggest that individuals with low registry processing demonstrate features that are simi- lar to those of individuals with a low neurological threshold, which include higher levels of distress, somatization, preoccu- pation with the body, anxiety, negative self-esteem and proble- ms at work. In addition, similarly to the correlations found re- garding the low neurological threshold, as the low registry sen- sory processing is more profound, somatization, distress, wea- ker ego strength, social deviance, a tendency for poignancy, an- xiety, thought disorders that stem from distress and social in- troversion are more likely to occur. These findings add a new aspect to the existing theoretical knowledge and emphasize the significance of understanding the psychological difficulties that characterize individuals with low registry processing. In addition, the similarity between the fea- tures of individuals with a high neurological threshold and a passive response strategy and individuals with a low neurolo- gical threshold and a passive response strategy might suggest a mixed model of abnormal sensory processing. It seems that the primary difficulty of some individuals with abnormal sensory processing is regulating the sensory processing, so that they oscillate between low and high neurological thresholds. This results in lower social skills. A study that examined the rela- tionship between sensory processing and disorders of the autis- tic spectrum, found that 60% of the individuals with autis- tic-spectrum disorders demonstrated higher scores on more than one sensory processing type. The authors argued that disorders on the autistic spectrum are related to abnormal sensory proc- essing of both kinds (sensory hyposensitivity and sensory hy- persensitivity), so that the sensory processing disruption stems from regulation difficulties and oscillations between high and low neurological thresholds (Crane, Goddard, & Pring, 2009). Thus, individuals with a passive behavioral response seem to be most susceptible to these regulation difficulties. Sensory Seeki n g Pr o fi l e : High Neurolo gi cal Threshold and Active Behavioral Response High-scorers on Sensory Seeking are characterized by low tendency for social introversion and extravagant characteristics. Moreover, the stronger the tendency for sensory seeking, there is less probability for depressive symptoms. These findings su- ggest that people with sensory seeking profile may not experi- ence stress, which is consistent with previous studies on this processing type (Miller, Anzalone, Lane, Cermak, & Osten, 2007). Several studies found that there is a connection between the intention and will to take part in high-risk sports activities and the need for physiologic stimulation (Diehem & Armatas, 2004; Franques et al., 2003; Shoam, Rose, & Kahle, 1998). Demoralization and Sensory Processing One of the most important common factors in the MMPI-2 is Copyright © 2012 SciRes 75  N. BEN-AVI ET AL. “Demoralization” (Almagor & Koren, 2001; Tellegen et al., 2003). Demoralization is experienced as a persistent inability to cope, together with associated feelings of helplessness, hope- lessness, meaninglessness, subjective incompetence and dimin- ished self-esteem. It was found that this factor has a major con- tribution on vast majority of the major psychological disorders measured by the MMPI-2 (Almagor & Koren, 2001, Tellegen et al., 2003). The work of Tellegen and associates (2003, 2008) provide strong evidence for the prominence of demoralization in understanding the nature of psychological disorders. In the current study, it is clear that demoralization and introversion plays a key factor in explaining the findings. Recent studies have found significant correlations between SPD and psychological difficulties among healthy adults. Engel- Yeger & Dunn (2011a) demonstrated how anxiety (trait anxiety and state anxiety) is related to extreme sensory processing pat- tern. Another study by Engel-Yeger & Dunn (2011b) revealed the connection between SPD and positive/negative Affect when negative affect correlated with Sensory Sensitivity, Sensory Avoiding and Low Registration and positive affect correlated with sensory seeking. Theses finding are consistent with the re- sult of the current study, suggesting the important role of sen- sory processing in psychological and interpersonal difficulties. Conclusion Clinically, the current study contributes to the understanding of how sensory processing in everyday life relates to psycho- logical experiences and behavior. Our findings do not support Dunn’s sensory processing mo- del. The psychological and social difficulties were related to three of the sensory processing types. These findings suggest that a bipolar model of sensory processing with regard to psy- chological and social difficulties may be a more precise one. Limitations the Study In order to examine the nature of the sensory processing, the current study used a self report questionnaire that examines behaviors after an encounter with sensory stimuli. Future stud- ies on the sensory processing and clinical features subject that will use physiological measures that evaluate directly, objec- tively and measurably the reaction to sensory stimuli, will be able to strengthen the validity of the findings in this study. The current study examined the sensory processing patterns in a distinct manner. As aforesaid, it may be that in certain con- ditions, the sensory processing disturbance stems from regula- tion difficulties and therefore it is expressed by oscillations between a high neurological threshold and a low one. Future studies in the field, that will be conducted on larger samples and on more varied populations as far as age and clinical syn- dromes are concerned, can investigate in a more focused man- ner the possible oscillations in the sensory functioning. The current study is a correlation study, and therefore it can- not be indicative of causal relations between sensory processing defects and clinical features. However, it is important to indi- cate that sensory processing defects are neurological defects, so it is likely that they form the ground for the development of the personality, in an interaction with environmental factors, of course. It can also be assumed that the relationship is not unidi- rectional and that the developing clinical features contribute to the development of the neurological defects. Future studies in the field can examine the influence of sensory processing diffi- culties on the development of the personality. In addition, more studies are needed regarding the interaction between sensory processing defects and environmental variables in the predic- tion of psychological difficulties and clinical features. The findings indicate that individuals with an increased tendency for sensory avoidance suffer from higher levels of stress (A), suffer more from a sense of alienation from themselves and others (Si2), have lower self-esteem (LSE), and social discomfort (SOD). They also suffer from a higher general level of distress (A), family problems (MDS) and less ego strength (ES). Acknowledgements We wish to acknowledgement the help of Prof. Danny Koren in commenting on an early draft of the study. REFERENCES Aron, E. N., & Aron, A. (1997). Sensory-processing sensitivity and its relation to introversion and emotionality. Journal of Personality and Social Psychology, 73, 345-368. doi:10.1037/0022-3514.73.2.345 Aron, E. N., Aron, A., & Davies, K. M. (2005). Adult shyness: The interaction of temperamental sensitivity and an adverse childhood environment. Personality and Social Psychology Bulletin, 31, 181- 197. doi:10.1177/0146167204271419 Almagor, M. (2005). The Hebrew Minnesota multiphase personality inventory-2. Jerusalem, Israel: Psych-Tech. (In Hebrew). Almagor, M., & Koren, D. (2001). The adequacy of the MMPI-2 har- ris-lingoes subscales: A cross-cultural factor analytic study of scales D, Hy, Pd, Sc and Ma. Psychological Assessment, 13, 199-215. doi:10.1037//1040-3590.13.2.199 Ben-Porath, Y., & Tellegen, A. (2008). MMPI-2 RF™ (minnesota multiphasic personality inventory-2 restructured form™). Pearson Assessment Systems, Minneapolis: University of Minnesota Press. Ben-Porath, Y. S., & Tellegen, A. (2008). Empirical correlates of the MMPI-2 restructured clinical (RC) scales in mental health, forensic, and non-clinical settings: An introduction. Journal of Personality Assessment, 90, 119-121. doi:10.1080/00223890701845120 Brown, C., & Dunn, W. (2002). Adolescent/adult sensory profile. San Antonio, TX: Psychological Corporation. Butcher, J. N., Dahlstrom, W. G., Graham, J. R., Tellegen, A. & Kae- mmer, B. (1989). Manual for the restandardized Minnesota multi- phasic personality inventory: MMPI-2. Minneapolis: University of Minnesota Press. Cermak, S. A. (1998). The relationship between attention deficit and sensory integration disorders (Part Ι). Sensory Integration: Special Interest Section, 11, 1-2. Cheng, M., & Boggett-Carsjens, J. (2005). Consider sensory processing disorders in the explosive child: Case report and review. The Cana- dian Child and Adolescent Psychiatry Review, 14, 44-48. Chutroo, B. (2007). The drive to be whole: A developmental model inspired by Paul Schilder and Lauretta Bender in support of holistic treatment strategies. The Arts in Psychotherapy, 34, 409-419. doi:10.1016/j.aip.2007.08.006 Crane, L., Goddard, L., & Pring, L. (2009). Sensory processing in adults with autism spectrum disorders. Autism, 13, 215-228. doi:10.1177/1362361309103794 Diehem, R., & Armatas, C. (2004). Surfing: An avenue for socially ac- ceptable risk-taking, satisfying needs for sensation seeking and ex- perience seeking. Personality and Individual Differences, 36, 663- 677. Dunn, W. (1997). The impact of sensory processing abilities on the daily lives of young children and their families. Infants and Young Children, 9, 23-35. doi:10.1097/00001163-199704000-00005 Dunn, W. (1999). Sensory profile. San Antonio, TX: Psychological Corporation. Copyright © 2012 SciRes. 76  N. BEN-AVI ET AL. Copyright © 2012 SciRes 77 Dunn, W. (2001). The sensations of everyday life: Empirical, theoreti- cal, and pragmatic considerations. 2001 Eleanor Clarke Slagle lec- ture. The American Journal of Occupational Therapy, 55, 608-620. doi:10.5014/ajot.55.6.608 Engel-Yeger, B., & Dunn, W. (2011a). The relationship between sen- sory processing difficulties and anxiety level of healthy adults. Brit- ish Journal of Occupational Therapy, 74, 210-216. doi:10.4276/030802211X13046730116407 Engel-Yeger, B., & Dunn, W. (2011b). Exploring the relationship be- tween affect and sensory processing patterns in adults. British Jour- nal of Occupational Therapy, 74, 456-464. doi:10.4276/030802211X13182481841868 Eysenck, H. J. (1967). The biological basis of personality (pp. 100-117). Springfield, IL: Thomas. Franques, P., Auriacombe, M., Piquemal, E., Verger, M., Brisseau- Gi- menez, S., Grabot, D., & Tignol, J. (2003). Sensation seeking as a common factor in opioid dependent subjects and high risk sport prac- ticing subjects: A cross sectional study. Drug & Alcohol Dependence, 69, 121-126. Graham, J. (2005). MMPI-2: Assessing personality and psychopatho- logy (pp. 188-214). New York: Oxford University Press. Greene, R. L. (2010). The MMPI-2/MMPI-2-RF: An interpretive ma- nual (3rd ed.). New-Jersey: Prentice Hall. Kandel, E. R. (1991). Cellular mechanisms of learning and the biologi- cal basis of individuality. In E. R. Kandel, J. H. Schwartz, & T. M. Jessell (Eds.), Principles of neural science (3rd ed., pp 1009-1031). East Norwalk, CT: Appleton & Lange. Kinnealey, M., & Fuiek, M. (1999). The relationship between sensory defensiveness, anxiety, depression, and perception of pain in adults. Occupational Therapy I nte r na t i o nal, 6, 195-206. doi:10.1002/oti.97 Liss, M., Mailloux, J., & Erchull, M. J. (2008). The relationship be- tween sensory processing sensitivity, alexithymia, autism, depression, and anxiety. Personality and Individual Dif f erences, 45, 255-259. doi:10.1016/j.paid.2008.04.009 Liss, M., Timmel, L., Baxley, K., & Killingsworth, P. (2005). Sensory processing sensitivity and its relation to parental bonding, anxiety, and depression. Personality and Individual Differences, 39, 1429- 1439. doi:10.1016/j.paid.2005.05.007 McKinley, J. C., & Hathaway, S. R. (1944). The minnesota multiphasic personality inventory, V: Hysteria, hypomania, and psychopathic de- viate. Journal of Applie d Psychology, 28, 153-174. doi:10.1037/h0059245 Miller, L. J., Anzalone, M. E., Lane, S. J., Cermak, S. A., & Osren, E. T. (2007). Concept evolution in sensory integration: A proposed noso- logy for diagnosis. The American Journal of Occupational Therapy, 61, 135-140. doi:10.5014/ajot.61.2.135 Parush, S., Engel-Yeger, B., & Ben-Sason, A. (2006). Hebrew transla- tion of the adolescent/adult sensory profile. Jerusalem: The School of Occupational Therapy, The Hebrew University of Jerusalem. (In He- brew). Royeen, B. C. (1989). Touch inventory for elementary school-aged children . The American Journal of Occupational Therapy, 17, 155-159. Royeen, C. B., & Lane, S. J. (1991). Tactile processing and sensory defensiveness. In A. G. Fisher, E. A. Murray, & A. C. Bundy (Eds.), Sensory integration: Theory and practice (pp. 108-136). Philadelphia: F. A. Davis. Shoam, A., Rose, G. M., & Kahle, L. R. 1998). Marketing of risky sports: From intention to action. Journal of the Academy of Market- ing Science, 26, 307-321. Simeonsson, R. J., Leonardi, M., Lollar, D., Bjorck-Akesson, E., Hol- lenweger, J., & Martinuzzi, A. (2003). Applying the international classification of functioning, disability and health (ICF) to measure childhood disability. Disability and Rehabilitation, 25, 602-610. doi:10.1080/0963828031000137117 Sutker, P. B., Archer, R. P., & Allain, A. N. (1978). Drug abuse pat- terns, personality characteristics, and relationships with sex, race, and sensation seeking. Journal of Counseling and Clinical Psychol- ogy, 46, 1374-1378. doi:10.1037//0022-006X.46.6.1374 Tal-Saban, M., Yochman, A., & Parush, S. (2002). Validity and reliability of the sensory profile in an Israeli population of children aged 3-6 years old. The Israel Journal of Occupational Therapy, 11, 33-48. (In Hebrew.) Tellegen, A., Ben-Porath, Y. S., McNulty, J. L., Arbisi, P. A., Graham, J. R.,& Kaemmer, B. (2003). MMPI-2 restructured clinical (RC) scales: Development, validation, and interpretation. Minneapolis: University of Minnesota Press. Ward, L. C., & Perry, M. S. (1998), Measurement of social introversion by the MMPI-2. Journal of Personality Assessment, 70, 171-182. Wilbarger, P., & Wilbarger, J. L. (1991). Sensory defensiveness in children aged 2-12. An intervention guide for parents and other caretakers. Santa Barbara: Avanti Educational Programs. Zuckerman, M., Bone, R. N., Neary, R., Mangelsdorff, D., & Brustman, B. (1972). What is the sensation seeker? Personality trait and ex- perience correlates of the sensation seeking scales. Journal of Coun- seling and Clinical Psychology, 39, 308-321. doi:10.1037/h0033398 Zuckerman, M., & Link, K. (1968). Construct validity for the sensation seeking scale. Journal of Counseling and Clinical Psychology, 32, 420-426. doi:10.1037/h0026047
|