Open Journal of Stomatology
Vol.3 No.1(2013), Article ID:29470,5 pages DOI:10.4236/ojst.2013.31017
An in vitro study of antimicrobial agents incorporated into interim restorative materials
![]()
1Department of Restorative Dentistry, University at Buffalo, School of Dental Medicine, Buffalo, USA
2Department of Periodontics and Endodontics, University at Buffalo, School of Dental Medicine, Buffalo, USA
Email: *jjzambon@buffalo.edu
Received 29 January 2013; revised 3 March 2013; accepted 13 March 2013
Keywords: Interim Restorations; Bis-Acryl Resin; Triclosan; Cetylpyridinium Chloride
ABSTRACT
Aim: To test the hypothesis that antimicrobial agents can be incorporated into bis-acryl resin and that the material will inhibit bacterial growth in vitro. Materials and Methods: 0.5%, 1% and 2% triclosan (5-chloro-2-(2,4-dichlorophenoxy)phenol) and 0.05% 0.01% and 0.15% cetylpyridinium chloride were incorporated into bis-acryl resins and molded into 1 mm × 10 mm discs. The discs were placed on bacterial culture media inoculated with Aggregatibacter actinomycetemcomitans strain Y4, Porphyromonas gingivalis strain SUNYaB A7A1-28 or Streptococcus gordonii strain 10558, incubated and examined for growth inhibition. Results: Triclosan-containing bisacryl resin discs produced dose-dependent zones of growth inhibition for A. actinomycetemcomitans but not S. gordonii or P. gingivalis. Cetylpyridinium chloride-containing discs produced dose-dependent zones of growth inhibition for Porphyromonas gingivalis and Streptococcus gordonii but not A. actinomycetemcomitans. Conclusion: Triclosan and cetylpyridinium chloride can be incorporated into bis-acryl resin and can inhibit the growth of plaque bacteria in a dose dependent manner. Bis-acryl resin containing antimicrobial agents may inhibit in vivo plaque accumulation and gingival inflammation.
1. INTRODUCTION
Interim restorations protect pulp, prevent dental caries, and maintain or improve function and esthetics. However, interim restorations accumulate oral biofilms resulting in gingival inflammation and even tooth decalcification. To prevent these sequelae, antimicrobial agents are sometimes incorporated into interim materials. For example, TempBond® ClearTM with Triclosan: Temporary Crown and Bridge Cement (Kerr Corporation, Orange, CA, USA) is a temporary cement containing 5-chloro-2-(2,4- dichlorophenoxy phenol (triclosan) [1]. Systemp. inlay (Ivoclar Vivadent, Amherst, NY, USA) also contains triclosan offering advantages as described on the product website, “Antimicrobial agents and reduction of undesirable odours” [2]. However, it is unclear if these triclosan-containing materials inhibit plaque accumulation [3].
Antimicrobial agents have been incorporated into a variety of dental materials including orthodontic adhesives [4], denture base materials [5], and dentinal bonding agents [6]. Rathke et al. [7] reported that resin composite containing 0.3% triclosan inhibited the in vitro growth of Streptococcus mutans, Actinomyces viscosus, and Lactobacillus casei. Sainulabdeen et al. [8] found that triclosan incorporated into glass ionomer cements was effective against Lactobacillus acidophilus and Streptococcus mutans. Namba et al. [9] found that the growth of S. mutans was significantly inhibited on the surface of resins containing 3% cetylpyridinium chloride. Imazato et al. [10] showed that composite incorporating 1% triclosan inhibited both the growth and adherence of S. mutans.
There are three types of materials commonly used to fabricate interim restorations—methacrylate, preformed materials and composite with the latter divided into bisacryl, bis-gma, and urethane resins.
This study tested the null hypothesis—antimicrobial agents can not be incorporated into bis-acryl resins used to fabricate interim restorations and antimicrobial-containing resins can not inhibit bacterial growth in vitro.
2. MATERIALS AND METHODS
2.1. Fabrication of Discs
Two different types of bis-acryl resins were used in this study—Systemp.onlay which contains polyesterurethane dimethacrylate, ethyl triglycol methacrylate, silica, copolymers, catalysts, pigments, and triclosan [11] and TempBond Clear which contains urethane diacrylate ester monomers (Kerr Corporation Orange, CA, USA). Two different antibacterial agents were used in this study—triclosan (Irgasan, Sigma-Aldrich Co. LLC) and cetylpyridinium chloride (Sigma-Aldrich Co. LLC). Triclosan was added at concentrations of 0.5%, 1%, and 2% (dry weight) and cetylpyridinium chloride was added at concentrations of 0.05%, 0.01%, and 0.15% (dry weight) based on previous studies [8,9].
Bis-acryl composite consisting of base and catalyst was extruded onto mixing paper, weighed and either triclosan or cetylpyridinium chloride was added. The base, catalyst and antimicrobial agent were mixed, loaded into a disposable syringe and dispensed into silicone molds. The resulting discs measured 10 mm in diameter by 1 mm thick. The disks were placed in sterile bags and autoclaved. Thirty disks were fabricated for each concentration and material as well as 30 control disks of each material without added antimicrobial agent.
2.2. Bacterial Strains and Testing
Representative oral bacteria were used to assess the antibacterial activity of the discs. They included Aggregatibacter actinomycetemcomitans, strain Y4—a gram negative capnophilic, coccobacillus originally isolated from subgingival plaque in a patient with localized aggressive periodontitis [12,13]; Porphyromonas gingivalis strain SUNYaB A7A1-28, a gram negative anaerobic rod originally isolated from subgingival plaque in a diabetic patient with chronic periodontitis [14] (University at Buffalo, School of Dental Medicine Culture Collection, Buffalo, NY, USA); and Streptococcus gordonii strain ATCC (American Type Culture Collection, Manassas, Virginia, USA) 10558 [15]—a gram positive aerobic rod which is one of the initial colonizers in dental plaque/oral biofilm formation.
All microorganisms were maintained on tryptic soy agar supplemented with 5% defibrinated sheep blood, 5.0 μg·ml−1 hemin, and 0.5 μg·ml−1, vitamin K1 (enriched tryptic soy agar, ETSA). Bacteria were harvested from 48 - 72 hr. cultures, dispersed in brain heart infusion broth (Becton, Dickinson and Company, Franklin Lakes, NJ USA 07417) and diluted to an OD660nm = 0.1. Aliquots of each test microorganism were distributed onto ETSA using a sterile cotton applicator.
Each ETSA plate was divided into three sections. In separate sections, we placed three control disks, disks containing 0.5%, 1%, and 2% added triclosan and disks containing 0.05%, 0.1%, 0.15% cetylpyridinium chloride (Figure 1). ETSA plates inoculated with either A. actinomycetemcomitans or S. gordonii were incubated at 35˚C -
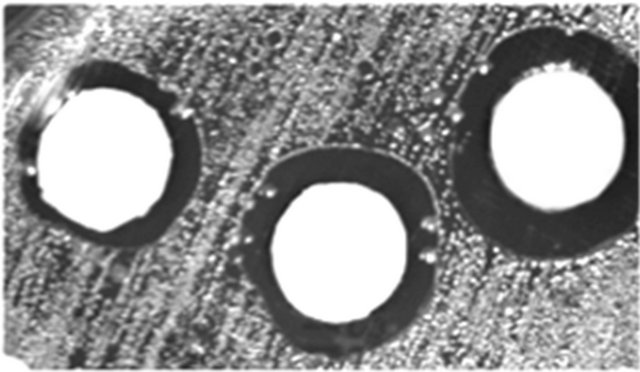
Figure 1. Zones of P. gingivalis growth inhibition around Temphase disks containing (from left to right) 0.05%, 0.01%, and 0.15% cetylpyridinium chloride.
37˚C in an atmosphere of 5% CO2 in air for 5 days. ETSA plates inoculated with P. gingivalis were incubated at 35˚C - 37˚C in an anaerobic chamber (Forma Scientific Inc., Marietta, Ohio) containing 5% CO2, 10% H2 and 85% N2 for 5 days.
Following incubation, the plates were examined for zones of inhibition with 3× magnification loupes. Measurements were made from the edge of the test disk to the zone of inhibition for all samples that produced a reaction.
2.3. Statistical Analysis
Separate two-way analysis of variance was used to evaluate differences in the size of the zones of inhibition. Tukey multiple comparisons were used to evaluate differences between mean pairs.
3. RESULTS
Both Systemp and Temphase bis-acryl resin disks containing 0.5%, 1% or 2% triclosan inhibited the growth of A. actinomycetemcomitans Y4 but not S. gordonii 10558 or P. gingivalis strain SUNYaB A7A1-28 (Table 1).
Both Systemp and Temphase bis-acryl resin disks containing 0.05%, 0.1% or 0.15% cetylpyridinium chloride inhibited the growth of S. gordonii 10558 and P. gingivalis SUNYaB A7A1-28 but not A. actinomycetemcomitans Y4 (Figure 1, Table 1).
Growth inhibition for both antimicrobial agents incorporated into either interim restorative material was dose dependent (Figure 2). That is, the zones of inhibition for triclosan tested against A. actinomyctemcomitans strain Y4 were larger at the highest concentration, 2.0%, than at the lower concentrations. Similarly for cetylpyridinium chloride, the zones of inhibition against P. gingivalis strain SUNYaB A7A1-28 and S. gordonii strain 10588 were larger at the highest concentration, 0.15%, than at the lower concentrations. None of the control disks produced zones of inhibition.
Table 1. Antibacterial effects of triclosan and CPC.

aA. actinomycetemcomitans strain Y4; bP. gingivalis strain SUNYaB A7A1- 28; cS. gordonii strain 10558; d Zone of growth inhibition present (+) or absent (−).
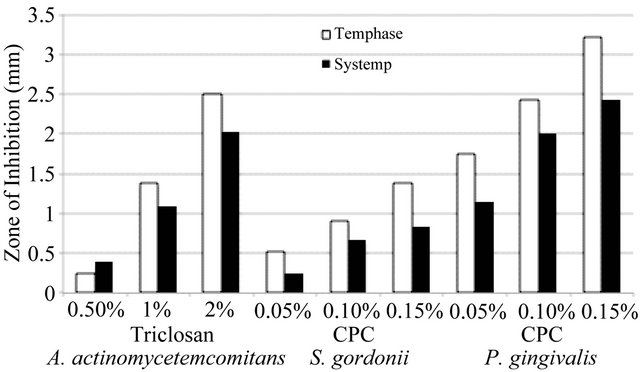
Figure 2. Growth inhibition by triclosan and cetylpyridinium chloride (CPC) incorporated into interim restorative materials.
For the bis-acryl resin with cetylpyridinium chloridetested against S. gordonii and P. gingivalis, two-way analysis of variance showed significant main effects for both the bis-acryl resin and for cetylpyridinium chlorideconcentration. There were greater mean zones of inhibition for Temphase than for Systemp.
Analysis of variance revealed a significant interaction between both bis-acryl resin interim restorative materials and the concentration of either triclosan or cetylpyridinium chloride. For triclosan inhibition of A. actinomycetemcomitans, p = 0.025. For cetylpyridinium chloride inhibition of P. gingivalis, p = 0.029 and for inhibition of S. gordonii, p = 0.029. Multiple comparisons (Tukey) showed significantly greater zones of inhibition for Temphase containing either triclosan or cetylpyridinium chloride than for Systemp containing either triclosan or cetylpyridinium chloride at higher concentrations, but there were no significant differences between the two interim materials at the lowest concentration of triclosan (0.5%) or cetylpyridinium chloride (0.05%). Temphase with cetylpyridinium chloride tested against P. gingivalis showed the greatest antibacterial effect.
4. DISCUSSION
Interim materials are porous and remain somewhat rough even after careful preparation. This leads to dental plaque accumulation, gingival inflammation and tooth demineralization especially if the interim restorations are placed for an extended period of time. However, biofilm formation is not restricted to the oral cavity. Biofilms accumulate on a variety of medical devices including central venous catheters, heart valves, ventricular assist devices, coronary stents, fracture-fixation devices, cochlear implants, and intraocular lenses [16].
Consequently, the desire to inhibit biofilms has stimulated the development of a variety of devices and materials containing antibacterial agents [17]. In the present study, we chose to test two antibacterial agents commonly used in dental products—cetylpyridinium chloride and triclosan. Cetylpyridinium chloride is a quaternary ammonium salt effective against a broad spectrum of oral bacteria [18]. It disrupts bacterial cell metabolism thereby inhibiting cell growth [19]. Triclosan is a synthetic, nonionic, broad spectrum antimicrobial agent effective against gram negative and gram positive bacteria [20]. One but not its only mode of antibacterial activity is to interfere with bacterial fatty acid synthesis leading to defective cell membranes [21].
The safety and efficacy of cetylpyridinium chloride and triclosan in the oral cavity have been repeatedly demonstrated. Haps et al. [22] reported that cetylpyridinium chloride mouthrinses reduce plaque and gingival inflammation when used as adjuncts to oral hygiene. Sreenivasan et al. [23] reported that mouthrinses containing 0.05% cetylpyridinium chloride demonstrated broadspectrum antimicrobial activity against both laboratory strains and supragingival plaque bacteria compared to a control mouthrinse without cetylpyridinium chloride. A six-month clinical trial by Mankodi et al. [24] found that a 0.07% cetylpyridinium chloride mouthrinse significantly reduced plaque, gingival inflammation and gingival bleeding. Similarly for triclosan, a 0.3% triclosan dentifrice demonstrated 36% less supragingival calculus compared to a 0.24% sodium fluoride control dentifrice [25]. Zambon et al. [26] examined 159 subjects over one year for oral microbial changes following the use of a 0.3% triclosan 2% Gantrez copolymer and 0.243% sodium fluoride dentifrice and found that continued use was associated with beneficial alterations in the bacterial composition of supragingival dental plaque without shifts towards triclosan resistant bacteria. Sreenivasan et al. [27] examined 120 adults with dental implants and found that subjects using a 0.3% triclosan 2% Gantrez copolymer and 0.243% sodium fluoride dentifrice demonstrated significantly lower levels of dental plaque, gingivitis, and bleeding on probing compared to a fluoride group and harbored significantly fewer Gram-negative anaerobes and >90% reductions in A. actinomycetemcomitans, Campylobacter rectus, Eubacterium saburreum, Fusobacterium nucleatum, P. gingivalis, Prevotella melaninogenica, Solobacterium moorei, and Tannerella forsythia.
The present study found that addition of either cetylpryridinium chloride or triclosan to interim materials can exert an antibacterial effect. There were several factors that might have influenced the results of this study. First, the antibacterial agents were manually mixed into the bis-acryl resin base and catalyst. This might have resulted in uneven distribution of the antibacterial agent in the bis-acryl resin which could account for the asymmetric zones of inhibition. A second factor relates to the fact that the oral cavity harbors billions of micro-organisms representing hundreds of different species [28]. Only three strains of three species were tested in this study although they included gram positive and gram negative aerobic, anaerobic and facultative oral bacteria. The two antibacterial agents—cetylpyridinium chloride and triclosan—were tested on only two bis-acryl composites. These same agents might perform differently if incorporated into other types of interim materials.
The results of the current study can be compared with a previous report of the antibacterial properties of Systemp [11]. In that study, 10 mm diameter by 2 mm thick Systemp.inlay disks developed 12.7 mm zones of inhibition in agar diffusion assays including the 10 mm diameter of the disc, that is, a 1.35 mm zone of inhibition from the edge of the disk against both Streptococcus mutans and Klebsiella pneumoniae. In the present study, 10 mm diameter by 1 mm thick Systemp.onlay control disks (without added antimicrobial agents) did not inhibit the growth of A. actinomycetemcomitans, P. gingivalis or S. gordonii. Differences in bacterial test strains—S. mutans and K. pneumoniae in the former study versus A. actinomycetemcomitans, P. gingivalis and S. gordonii in the present study—may account for differences between the two studies. Also, the greater thickness of test disks in the former study—2 mm vs 1 mm in the present study—could account for the growth inhibition noted in that study and the lack of inhibtion noted in the control disks in the present study. Support for this idea—that greater amounts of Systemp might release greater amounts of triclosan—can also be found in the former study. Systemp.inlay and Systemp.onlay restorations were removed from patients and assayed for cariogenic and odor-forming bacteria. The study reported that the triclosan-containing interim materials did, “… not completely suppress the growth of bacteria… [but] cariogenic and odour-forming microorganisms could no longer be identified.”
Further research is needed to assess the physical properties of the modified bis-acryl resins to ensure that the antibacterial-composite mixture has adequate strength even though the intended use is not permanent but interim restorations. Previous studies have shown significant reductions in the compressive strength of glass ionomer cements to which antibacterial agents have been added although this effect appears to be minimal at low concentrations [29,30] and may meet acceptable hardness standards [31].
Within the limitations of this study, we conclude that cetylpyridinium chloride and triclosan can be incorporated into bis-acryl interim restorative materials where they can exert dose dependent antibacterial effects against oral bacteria. Since neither agent was effective against all test strains, it may be useful to combine agents to enhance the antibacterial effect.
5. ACKNOWLEDGEMENTS
We thank Carol Parker for assistance with the microbiological assays.
![]()
![]()
REFERENCES
- Kerr Dental (2012) TempBond, TempBond NE, and TempBond Clear with Triclosan temporary dental cement. http://www.kerrdental.com/kerrdental-temporization-tempbond-ne-clear-2
- IvoclarVivadent. (2012) Systemp.inlay/Systemp.onlay. http://www.ivoclarvivadent.us/en-us/all-products/temporary-filling-materials/systemp_inlay-_-systemp_onlay
- Slutzky, H., Slutzky-Goldberg, I., Weiss, E.I. and Matalon, S.M. (2006) Antibacterial properties of temporary filling materials. Journal of Endodontics, 32, 214-217.
- Chin, M.Y., Sandham, A., Rumachik, D.N., Ruben, J. L., and Huysmans, M.C. (2009) Fluoride release and cariostatic potential of orthodontic adhesives with and without daily fluoride rinsing. American Journal of Orthodontics and Dentofacial Orthopedics, 136, 547-553. doi:10.1016/j.ajodo.2007.10.053
- Kamijo, A.K., Mukai, Y., Tominaga, T., Iwaya, I., Fujino, F., Hirata, Y. and Teranaka, T. (2009) Fluoride release and recharge characteristics of denture base resins containing surface pre-reacted glass-ionomer filler. Dental Materials Journal, 28, 227-233. doi:10.4012/dmj.28.227
- Cheng, L., Zhang, K., Melo, M.A., Weir, M.D., Zhou, X. and Xu, H.H. (2012) Anti-biofilm dentin primer with quaternary ammonium and silver nanoparticles. Journal of Dental Research, 91, 598-604. doi:10.1177/0022034512444128
- Rathke, A., Staude, R., Muche, R. and Haller, B. (2010) Antibacterial activity of a triclosan-containing resin composite matrix against three common oral bacteria. Journal of Materials Science: Materials in Medicine, 21, 2971- 2977. doi:10.1007/s10856-010-4126-1
- Sainulabdeen, S., Neelakantan, P., Ramesh, S. and Subbarao, C.V. (2010) Antibacterial activity of triclosan incorporated glass ionomer cements—An in vitro pilot study. Clinical Pediatric Dentistry, 35, 157-161.
- Namba, N., Yoshida, Y., Nagaoka, N., Takashima, S., Matsuura-Yoshimoto, K., Maeda, H., Van Meerbeek, B., Suzuki, K. and Takashiba, S. (2009) Antibacterial effect of bactericide immobilized in resin matrix. Dental Materials, 25, 424-430. doi:10.1016/j.dental.2008.08.012
- Imazato, S., Torii, M. and Tsuchitani, Y. (1995) Antibacterial effect of composite incorporating triclosan against Streptococcus mutans. Journal of the Osaka University Dental School, 35, 5-11.
- IvoclarVivadent AG R&D/Scientific Service (2001) Scientific documentation: Systemp®.inlay, Systemp®.onlay.
- Newman, M.G., Socransky, S.S., Savitt, E.D., Propas, D.A. and Crawford, A. (1976) Studies of the microbiology of periodontosis. Journal of Periodontology, 47, 373- 379. doi:10.1902/jop.1976.47.7.373
- Tanner, A.C., Haffer, C., Bratthall, G.T., Visconti, R.A. and Socransky, S.S. (1979) A study of the bacteria associated with advancing periodontitis in man. Journal of Clinical Periodontology, 6, 278-307. doi:10.1111/j.1600-051X.1979.tb01931.x
- Zambon, J.J., Reynolds, H., Fisher, J.G., Shlossman, M., Dunford, R. and Genco, R.J. (1988) Microbiological and immunological studies of adult periodontitis in patients with noninsulin-dependent diabetes mellitus. Journal of Periodontology, 59, 23-31. doi:10.1902/jop.1988.59.1.23
- Kilian, M., Mikkelsen, L. and Henrichsen, J. (1989) A study of viridans streptococci: Description of Streptococcus gordonii sp. nov. and emended descriptions of Streptococcus sanguis (White and Niven 1946), Streptococcus oralis (Bridge and Sneath 1982), and Streptococcus mitis (Andrewes and Horder 1906). International Journal of Systematic Bacteriology, 39, 471-484. doi:10.1099/00207713-39-4-471
- Costerton, W., Montanaro, L. and Arciola, C.R. (2005) Biofilm in implant infections: Its production and regulation. International Journal of Artificial Organs, 28, 1062- 1068.
- Brooks, B.D., Brooks, A.E. and Grainger, D.W. (2012) Antimicrobial medical devices in preclinical development and clinical use. In: Moriarty, T.F., Zaat, S.A.J. and Busscher, H.J., Eds., Biomaterials Associated Infection: Immunological Aspects and Antimicrobial Strategies, Springer, New York, 307-354.
- Wu, C.D. and Savitt, E.D. (2002) Evaluation of the safety and efficacy of over-the-counter oral hygiene products for the reduction and control of plaque and gingivitis. Periodontology, 28, 91-105. doi:10.1034/j.1600-0757.2002.280105.x
- Denyer, S.P. and Stewart, G.S.A.B. (1998) Mechanisms of action of disinfectants. International Biodeterioration and Biodegradation, 41, 261-268. doi:10.1016/S0964-8305(98)00023-7
- Bhargava, H.N. and Leonard, P.A. (1996) Triclosan: Applications and safety. American Journal of Infection Control, 24, 209-218. doi:10.1016/S0196-6553(96)90017-6
- Heath, R.J., Rubin, J.R., Holland, D.R., Zhang, E., Snow, M.E. and Rock, C.O. (1999) Mechanism of triclosan inhibition of bacterial fatty acid synthesis. Journal of Biological Chemistry, 274, 11110-11114. doi:10.1074/jbc.274.16.11110
- Haps, S., Slot, D.E., Berchier, C.E. and Van der Weijden, G.A. (2008) The effect of cetylpyridinium chloride-containing mouth rinses as adjuncts to toothbrushing on plaque and parameters of gingival inflammation: A systematic review. International Journal of Dental Hygiene, 6, 290-303. doi:10.1111/j.1601-5037.2008.00344.x
- Sreenivasan, P.K., Haraszthy, V.I. and Zambon, J.J. (2012) Antimicrobial efficacy of 0.05% cetylpyridinium chloride mouthrinses. Letters in Applied Microbiology, 56, 14-20. doi:10.1111/lam.12008
- Mankodi, S., Bauroth, K., Witt, J.J., Bsoul, S., He, T., Gibb, R., Dunavent, J. and Hamilton, A. (2005) A 6- month clinical trial to study the effects of a cetylpyridinium chloride mouthrinse on gingivitis and plaque. American Journal of Dentistry, 18, 9A-14A.
- Lobene, R.R., Battista, G.W., Petrone, D.M., Volpe, A.R. and Petrone, M.E. (1991) Clinical efficacy of an anticalculus fluoride dentifrice containing triclosan and a copolymer: A 6-month study. American Journal of Dentistry, 4, 83-85.
- Zambon, J.J., Reynolds, H.S., Dunford, R.G., DeVizio, W., Volpe, A.R., Berta, R., Tempro, J.P. and Bonta, Y. (1995) Microbial alterations in supragingival dental plaque in response to a triclosan-containing dentifrice. Oral Microbiology and Immunology, 10, 247-255. doi:10.1111/j.1399-302X.1995.tb00150.x
- Sreenivasan, P.K., Vered, Y., Zini, A., Mann, J., Kolog, H., Steinberg, D., Zambon, J.J., Haraszthy, V.I., da Silva, M.P. and DeVizio, W. (2011) A 6-month study of the effects of 0.3% triclosan/copolymer dentifrice on dental implants. Journal of Clinical Periodontology, 38, 33-42. doi:10.1111/j.1600-051X.2010.01617.x
- Bik, E.M., Long, C.D., Armitage, G.C., Loomer, P., Emerson, J., Mongodin, E.F., Nelson, K.E., Gill, S.R., Fraser-Liggett, C.M. and Relman, D.A. (2010) Bacterial diversity in the oral cavity of 10 healthy individuals. ISME Journal, 4, 962-974. doi:10.1038/ismej.2010.30
- Botelho, M.G. (2004) Compressive strength of glass ionomer cements with dental antibacterial agents. South African Dental Journal, 59, 51-53.
- Dimkov, A., Nicholson, W.J., Gjorgievska, E. and Booth, S. (2012) Compressive strength and setting time determination of glass-ionomer cements incorporated with cetylpyridinium chloride and benzalkonium chloride. Prilozi, 33, 243-263.
- Tüzüner, T. and Ulusu, T. (2012) Effect of antibacterial agents on the surface hardness of a conventional glassionomer cement. Journal of Applied Oral Science, 20, 45-49. doi:10.1590/S1678-77572012000100009
NOTES
*Corresponding author.