17
H. ZHANG ET AL.
3. Disscusion
PCNL, due to its high success rate of stone clearance and
minimally invasive characteristics, has become the pre-
ferred method for renal and upper ureteral stones, espe-
cially the complex renal calcu li [2]. Despite the evidence
of its safety and efficacy either in adult and pediatric pa-
tients [3], or in pregn ant women [4], PCNL still beh aves
with some complications, including the damages on the
renal function. It was generally believed that the upper
urinary tract obstruction, infection and interstitial renal
scar caused by kidney stones, will eventu ally resu lt in the
damage of renal function. Segura and Liou et al. reported
that PCNL could effectively remove the stones and re-
lieve the obstruction, to maintain or even improve the re-
nal function [5,6]. Regarding to long-term effect, there are
several reports. Kuzgunbay et al. reported that most pa-
tients presenting with kidney-stome disease and ren al in-
sufficiency experience improvement or stabilization of renal
function after PCNL [7]. In another study, Kuzgunbay
et al. reported that patients underwent PCNL ia an ade-
quate treatment modality even in the presence of com-
plete staghorn calculi, comorbid diseases or previous ip-
silateral renal surgery [8]. In another study carried by
El-Nahas et al., it was reported that long-term functional
results of PCNL were satisfactory as 91.5% of kidneys
showed stable or improved GFR [9].
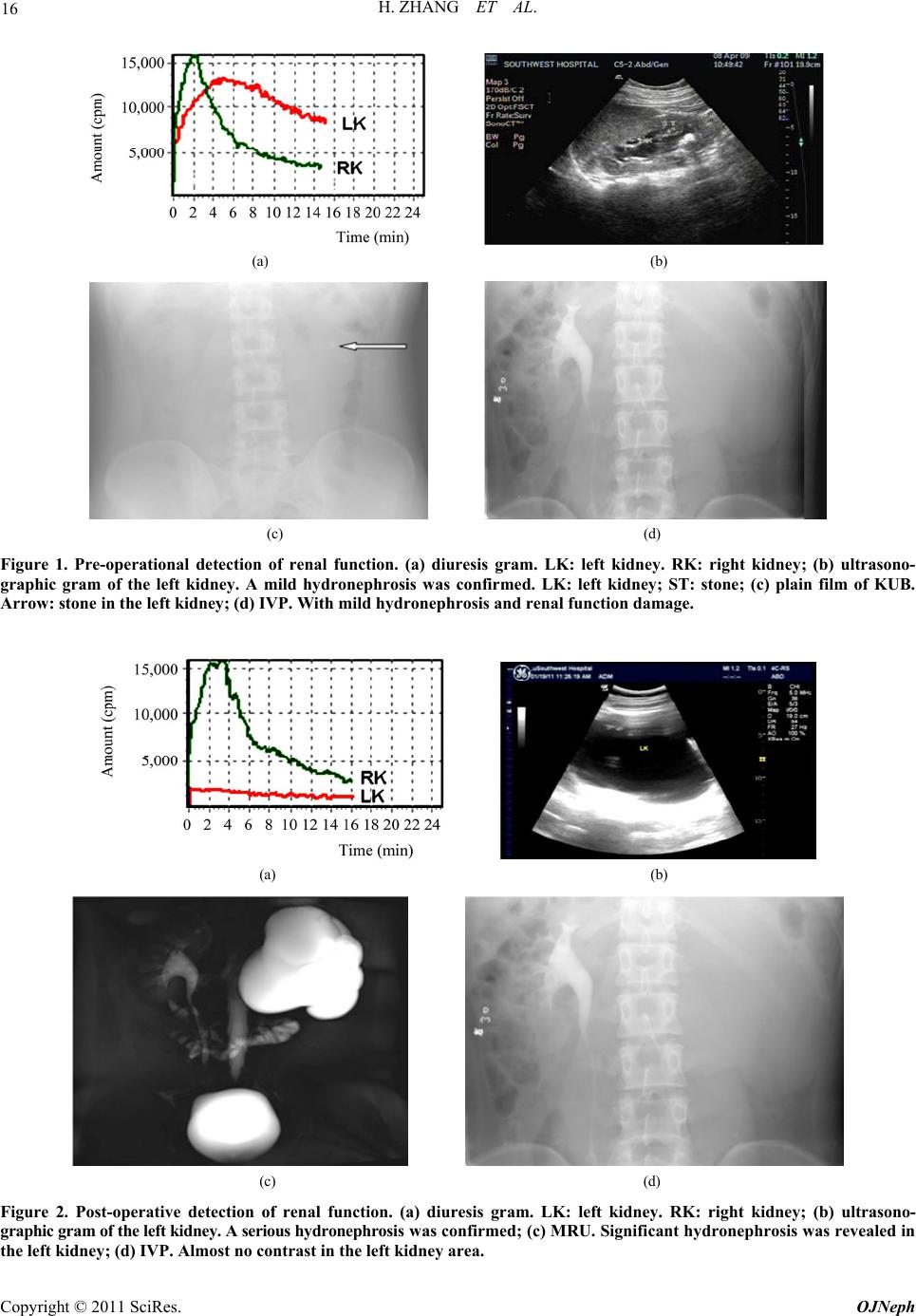
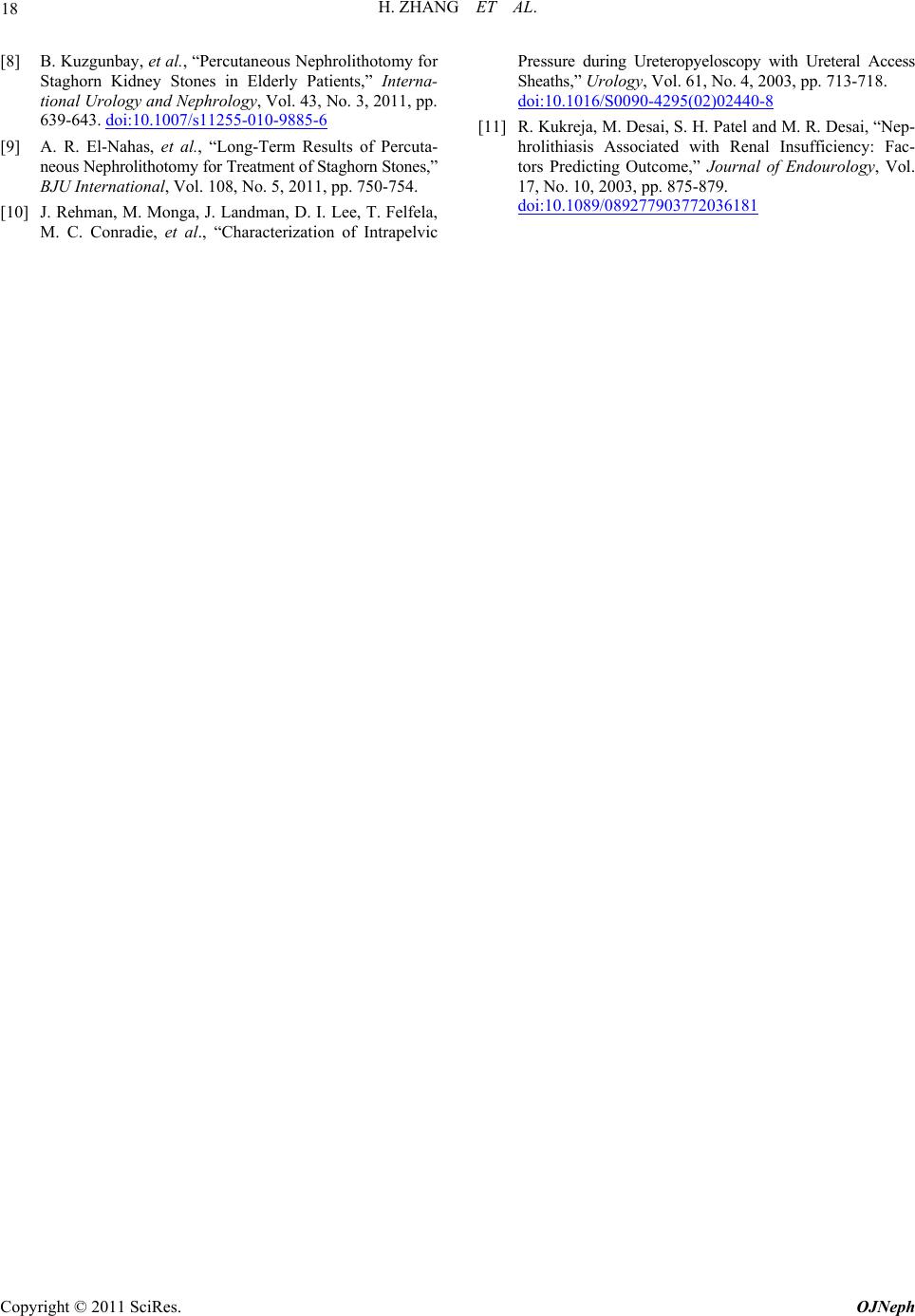
In this case, a serious deterioration of renal function
after percutaneous nephrolithotomy was confirmed. The
preoperative renal function had just mildly declined, but
almost completely lost after PCNL two years later, with-
out an y evidence of secondary ureteral obstruction, chron ic
ne phritis or nephrotic syndrome. Theoretically, there seems
to be some potential mechanisms associated with the renal
function deterioration, such as: 1) high internal renal pel-
vis pressure, due to the necessary pressure by irrigation
for high qualified observation view and stone removal
[10]. But when the perfusion pressure rises to 300 mmHg,
the intrapelvic pressure may rise to more than 40 cmH2O,
which may result in pyelosinus, pyelovenous, and/or pye-
lolymphatic backflow. 2) Injury of the laser energy. La-
ser could disintegrate the stone with delicacy, but could
result in the risk of perforation and injury to the urothe-
lium at the same time. 3) Potential func tional obstruction.
If the pelvis-uretheral junction was damaged, the ureteral
peristaltic movement might be depressed, which might
cause a secondary fun ctional obstru ction. 4) Ischemia-re-
perfusion injury. Once the renal interstitium edema gra-
dually increased, the pressure of interstitium would ex-
ceed that of the renal arteries, resulting in the renal ische-
mia-reperfusion injury, stagnation of artery blood flow
and formation of micro-thrombosis. Even the ischemic
renal necrosis and fibrosis, which influenced by stone
si ze, operation time, preoperative renal function, blood loss
and blood pressure control and so on, can cause the damage
to the renal function. Moreover, the renal function dete-
rioration was correlated with the long-time infection th at
caused by kidney stone, intraoperative mucosal injury,
residual stones and indwelling double-pigtail stent, which
may result in the chronic kidney inflammation and fibro-
sis [11]. Moreover, although the patient was diagnosed
without any metabolic adnormalities, he had not been deeply
checked up. These would remind us to pay attention to
the patients underwent PCNL.
In conclusion, PCNL is still considered as a safe and
effective endoscopic technique for urinary stones. But we
should pay more attention to preserve the renal function
in PCNL, including to adopt small tract, reduce p erfusion
pressure and bleeding, shorten operation time, control preo-
perative and postoperative urinary tract infections, and
maintain the patency of the urin ary drainage.
4. References
[1] M. S. Michel, L. Trojan and J. J. Rassweiler, “Complica-
ti o ns i n Percutaneous Nephrolithotomy,” European Urol ogy,
Vol. 51, No. 4, 2007, pp. 899-906.
doi:10.1016/j.eururo.2006.10.020
[2] R. Goel, M. Aron, P. K. Kesarwani, P. N. Dogra, A. K.
Hemal and N. P. Gupta, “Percutaneous Antegrade Re-
moval of Impacted Upper-Ureteral Calculi: Still the
Treatment of Choice in Developing Countries,” Journal
of Endourology, Vol. 19, No. 1, 2005, pp. 54-57.
doi:10.1089/end.2005.19.54
[3] A. R. El-Nahas, A. A. Shokeir, M. R. El-Kenawy, A. M.
Shoma, I. Eraky, A. M. El-Assmy, et al., “Safety and Ef-
ficacy of Supracostal Percutaneous Nephrolithotomy in
Pediatric Patients,” Journal of Endourology, Vol. 180, No.
2, 2008, pp. 676-680. doi:10.1016/j.juro.2008.04.046
[4] L. Khoo, K. Anson, U. Patel, “Success and Short-Term
Complication Rates of Percutaneous Nephrostomy during
Pregnancy,” Journal of Vascular and Interventional Ra-
diology, Vol. 15, No.12, 2004, pp. 1469-1473.
[5] J. W. Segura, D. E. Patterson, A. J. LeRoy, H. J. Wil-
liams Jr., D. M. Barrett, R. C. Benson Jr., et al., “Percu-
taneous Removal of Kidney Stones: Review of 1,000
Cases,” Journal of Endourology, Vol. 134, No. 6, 1985, pp.
1077-1081.
[6] L. S. Liou and S. B. Streem, “Long-Term Renal Func-
tional Effects of Shock Wave Lithotripsy, Percutaneous
Nephrolithotomy and Combination Therapy: A Compara-
tive Study of Patients with Solitary Kidney,” Journal of
Endourology, Vol. 166, No. 1, 2001, pp. 36-37.
doi:10.1016/S0022-5347(05)66070-3
[7] B. Kuzgunbay, et al., “Long-Term Renal Function and
Stone Recurrence after Percutaneous Nephrolithotomy in
Patients with Renal Insufficiency,” Journal of Endourol-
ogy, Vol. 24, No. 2, 2010, pp. 305-308.
doi:10.1089/end.2009.0362
Copyright © 2011 SciRes. OJNeph