Open Journal of Preventive Medicine
Vol.3 No.2(2013), Article ID:30920,7 pages DOI:10.4236/ojpm.2013.32034
Socio-maternal risk factors of ADHD among Iraqi children: A case-control study
![]()
1Department of Community Health, Universiti Kebangsaan Malaysia Medical Centre, Kuala Lumpur, Malaysia; *Corresponding Author: albayatihussain@yahoo.com
2Department of Family Medicine, University Malaya Medical Centre, Kuala Lumpur, Malaysia
Copyright © 2013 Hussain R. Saadi et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 16 January 2013; revised 12 March 2013; accepted 19 April 2013
Keywords: ADHD; Socio-Maternal; Risk factors; Case-control
ABSTRACT
Background: Attention-deficit hyperactivity disorder (ADHD) is a chronic disorder that appears first in childhood at preschool age (4 - 5) years, and is manifested by a symptomatic pattern of difficulties with attention, motor activity and impulsivity. Maternal factors like stress, sociodemographic and maternal life style factors are potential risk factors for ADHD. Methodology: A retrospective case-control study was conducted in Baghdad-Iraq. Cases have been taken from 5 private paediatric clinics. Controls were chosen from kindergartens within the same residential area of the paediatric private clinics. Mothers of cases and controls were investigated for the risk factors of ADHD using a self-administered questionnaire. The total sample size was 260. Number of cases was 130 and number of controls was 130. Results: Five variables were significantly associated with development of ADHD after using a multivariate logistic regression model, maternal war stress (Adjusted OR 9.08, 95% CI 4.70 - 17.52 and P value < 0.001), maternal smoking (Adjusted OR 3.27 95% CI 1.40 - 7.63, P < 0.001), father lost job (Adjusted OR 2.81, 95% CI 1.51 - 5.24, P value < 0.001), and house damaged (Adjusted OR 2.55, 95% CI 1.04 - 6.24, P < 0.05). Family income was also associated with risk of ADHD (OR 1.02 95% CI 1.00 - 3.12, P value < 0.05). Conclusion and suggestion: Maternal exposure to war stress has 9 times higher risk of developing ADHD among offspring. This study aimed to offer to the policy makers a good benchmark to plan more programmes related to women and child health with respect to the fourth and fifth Millennium Development Goals (MDGs) in reduction of child mortality and mor- bidity and improvement of maternal health. There is a real necessity to address the need of vulnerable pregnant mothers at war and disaster’s time for programmes which will be able to control the stress that those pregnant mothers would encounter during those hard times.
1. INTRODUCTION
Attention-deficit hyperactivity disorder (ADHD) is one of the most common mental disorders, affecting both children and adolescents with prevalence in no referred samples of 3% - 10% [1]. ADHD is also considered the most common cognitive and behavioral disorder diagnosed among school children) [2].
ADHD is a neurobehavioral disorder characterized by pervasive inattention and/or hyperactivity-impulsivity resulting in a significant functional impairment mainly problem solving, deficient attention along with hyperactivity and difficulty withholding incorrect answers [3].
Although, the prevalence of ADHD decreases with increasing age, symptoms persist throughout adulthood in about 50% of affected children [4].
If left untreated, the symptoms of ADHD can significantly affect a child’s academic and social functioning. Moreover, these symptoms have been shown to predispose patients to accidents due to their inattentive state. In general, there are 2 types of ADHD. These are the inattentive and hyperactive/impulsive types according to the Diagnostic and Statistical Manual of Mental Disorders, The Fourth Edition (DSM IV) [3].
In Iraq, Risk factors of ADHD have not been explored before. However, Prevalence of ADHD among schoolchildren in Baghdad (the capital of Iraq) is 10.5% [5]. Although, there is no general consensus regarding the etiology of ADHD, most investigators endorse a neural foundation to the origin of the disorder [6].
The etiology of ADHD is multifactorial. There are many factors whether directly or indirectly affecting the individual and can lead to the development of ADHD. In order to understand the etiology of ADHD we need to classify it into many risk factors which can cause ADHD. The mechanism by which maternal stress causes developmental problems in offspring is still unclear, but several hypotheses exist. Even though there are no direct connections between the maternal and foetal nervous systems, the mother’s emotional state can influence the foetus’s reactions and development [7].
It has been shown that, the activation of the sympathetic nervous system which, occurs during stress, causes an increase in uterine artery resistance that subsequently reduces blood flow to the fetus [7]. This decrease in blood flow to the fetus may impair the development of organs, including the brain of the fetus. Moreover, it has been shown that, although 50% - 90% of the cortisol which is released in the mother’s blood in response to maternal stress, is deactivated by special enzyme, a certain amount of cortisol can escape this deactivation and reaches the fetus [8]. By this mechanism, the increased fetal cortisol can alter the development of the baby’s nervous system and deregulate the hypothalamo-pituitary-adrenal (HPA) axis in the fetus, causing deregulated HPA response to stress in the child postnatally (ADHD like disorder).
In human being, gestational stress has been shown to be a potential factor associated with a higher risk to develop some neurological and psychiatric disorders. Similarly, in animal models, stress can induce lasting deficits in the offspring. Long-lasting effects of stress have been linked to disturbances in the function of the hypothalamo-pituitary-adrenocortical axis. Moreover, stress during pregnancy may cause alteration in brain development, leading to altered synaptic connectivity and persistent deficits in brain function [9].
A direct link between antenatal maternal mood and fetal behavior was observed by ultrasound from 27 to 28 weeks of gestation onwards [10]. Moreover, 14 independent prospective studies have shown a link between antenatal maternal anxiety or stress and cognitive, behavioural, and emotional problems in the child. This link generally persisted after controlling for postnatal maternal mood and other relevant confounders in the preand post-natal periods [11].
Stress following wars and disasters is considered capable of affecting pregnant mothers. In a study by Xiong et al. of 301 women from New Orleans and Baton Rouge, pregnant women were interviewed about their experiences during the hurricane, and whether they experienced symptoms of post-traumatic stress disorder (PTSD) or depression. In this study, “high hurricane exposure” was defined as having experienced 3 or more of the 8 severe hurricanes to have hit the area, having gone through the feeling that one’s life was in danger, have walked through floodwaters, or have had a loved one die.
The conclusion derived from that study was that women who have had high hurricane exposure were at an increased risk of having low birth weight infants. Rather than a general exposure to disaster, exposure to specific severe disaster events and the intensity of the disaster experience may be better predictors of poor pregnancy outcomes. It was suggested that to prevent poor pregnancy outcomes during and after disasters, future disaster preparedness may need to include the planning of earlier evacuation of pregnant women to minimize their exposure to severe disaster events [12].
The effects of natural disasters, war, and family violence on the mental health of 296 children and adolescents in Sri Lanka were studied. These children and adolescents (9 to 15 years old), who were exposed to civil war and the Asian Tsunami, completed a survey regarding war-related events, tsunami exposure, and family violence. Of those surveyed, 82% had experienced at least 1 war-related event in their lifetimes. The most common events were seeing a dead or mutilated body (44%), being close to a combat situation (40%), and witnessing gunfire or shelling (33%). Seventy-one percent of the children were directly affected by the tsunami; more than half had seen the wave close by; almost all had to flee; and about a quarter had been caught by the wave [13].
In another study, the efficacy of school-based intervention was assessed in a sample of 403 children (mean age, 10 years) who had been exposed to armed conflict in Central Sulawesi, Indonesia. These children had symptoms of PTSD and anxiety. They were randomized to a 15-session, school-based intervention or a wait-list control group. The intervention included cognitive-behavioral techniques, cooperative play, and creative-expressive elements (e.g., drama, dance, music).
Those in the school-based group had significantly more improvement in PTSD symptoms and increased hope than did those in the wait-list control group. However, stress-related physical symptoms, depressive symptoms, anxiety, and functioning did not differ between the treatment and wait-list control groups. The authors speculated that psychosocial intervention alone was not sufficient to counter the chronic poverty and political instability in the region. They suggested that poverty reduction and conflict resolution in addition to psychosocial intervention may be necessary to improve the mental health functioning of these children [14].
2. METHODS AND MATERIALS
In the present study, the aim was to include children of all types of ADHD as cases regardless what type of ADHD they are.
A total number of 260 participants were chosen for retrospective case-control study (one hundred and thirty cases and 130 controls). This study was carried out in Baghdad city (The Capital city of Iraq) where most of the war events in 2003 happened, which gives the researcher a great opportunity to assess the correlation between ADHD as a dependent variable of this study and maternal war stress and other independent variables like sociodemographic and maternal life style variables.
Baghdad city is a big city with nearly 6.5 million populations. It is a multiethnic, multinational and multi religious city which gives the researchers more freedom to generalize the findings.
Populations for this study were preschool children (4 - 6 years old) with their mothers along. Cases were chosen from 5 private pediatric clinics in districts of Baghdad city. Controls were chosen from 20 kindergartens within the same geographical zone of the private pediatric clinics. Cases were diagnosed as ADHD by consultant Pediatricians using the Diagnostic and Statistical Manual of Mental Disorders, form, the fourth edition (DSM IV).
Sampling method for cases was simple random sampling by choosing 130 children randomly from a pool containing 520 children diagnosed with ADHD. Sampling method or technique for controls was systematic sampling by choosing 130 names of 4 - 6 years old children from a list of 1300 children; each 10th name was chosen (systematic random sampling). Inclusion criteria were: children (4 - 6 years old), born and cared by their biological mothers, Iraqis, and their mothers are still alive to be contacted. Exclusion criteria were: Children who may have a history of other mental disorder like mental retardation or psychoses which might interact with ADHD diagnosis.
Mothers of cases and controls were contacted and were asked to sign consent forms participate in this study. Then a self-administered questionnaire was dispersed to all mothers. Response rate was 100%. The questionnaire contained questions related to sociodemographic characteristics of those mothers, maternal life style (mainly smoking and caffeine intake during pregnancy). Maternal stress questionnaire was developed based on some parts of the Harvard post-traumatic stress questionnaire (the Arabic version). The stress questionnaire included 10 very specific questions related to events or scenarios of wars. Each yes answer is given 1 point and no answer a zero point. Scoring for the stress is as following: 0 = No stress, 1 - 5 = mild-moderate stress, more than 5 is severe stress. In our study, we decided to consider the severe stress as a risk factor for ADHD. We did extra validation for the questionnaire and a pretest for the participants was done for 30 mothers to ensure that the questionnaire items were easily understood. Approval for this study was obtained from the pediatric private clinics and from the kindergarten’s management. The study was conducted between June-September 2008.
3. RESULTS
Table 1 shows sociodemographic and lifestyle distribution of study samples (N = 300).
The highest percentages of mothers enrolled in the study aged 25 - 33 (47.7% for mothers of cases and 46.2% for mothers of controls). Arabic mothers were the most participants compared to Kurdish and Turkman.
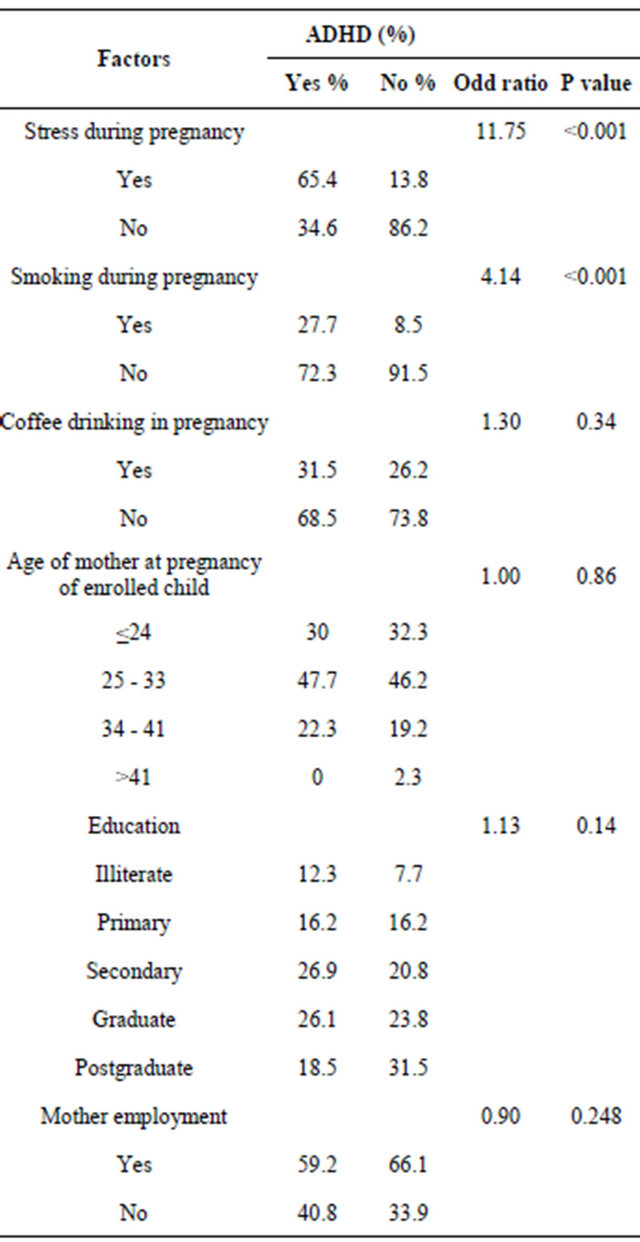
Table 2 shows that 65.4% of mothers of cases were significantly exposed to stress during pregnancy compared to only 13.8% of mothers of controls (P value < 0.001). This indicates that more mothers of ADHD children were exposed to stress during pregnancy than mothers of children who do not have ADHD.
There was about 27.7% of mothers of cases who were significantly exposed to cigarette smoking during pregnancy compared to only 8.5% of mothers of controls, (P value < 0.001). This means more mothers of ADHD children were smokers during pregnancy than mothers of children who do not have ADHD.
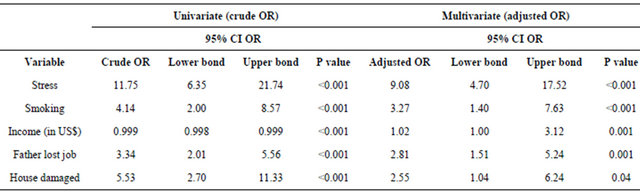
Table 3 shows univariate and multivariate logistic regression analyses. The full model included the 9 significant variables; income, stress, smoking, family member hit & injured, father lost the job and house damaged & relocate, family member hit at war family member died at war house damaged. After adjusting the effect of the independent variables, the final model included only five variable as shown below which gives Hosmer and Lemeshow Test P = 0.924 ( goodness of fit of the model).
Looking into the final model, the stress factor was independently significant, with an adjusted odd ratio of 9.08 (95%CI 4.70 - 17.52, P < 0.001). Smoking was also independently significant, with an adjusted odd ratio of 3.27 (95% CI 1.40 - 7.63 P < 0.001). The income variable had also a significant association with ADHD (adjusted OR 1.02 95%1.00 - 3.12, P < 0.001). Another independently significant variable was loss of father’s job with an adjusted odd ratio of 2.81 (95% CI 1.51 - 5.24 P < 0.001). The last independently significant variable was house damaged with an adjusted odd ratio of 2.55 (95% CI 1.04 - 6.22 P value < 0.05).
4. DISCUSSION
In this study, the aim was to investigate the effect of maternal exposure to war stress in Iraq on the pregnant mothers and whether this would be associated with hav-
Table 1. Distribution of selected sociodemographic and life style characteristics of mothers and children participating in the study.
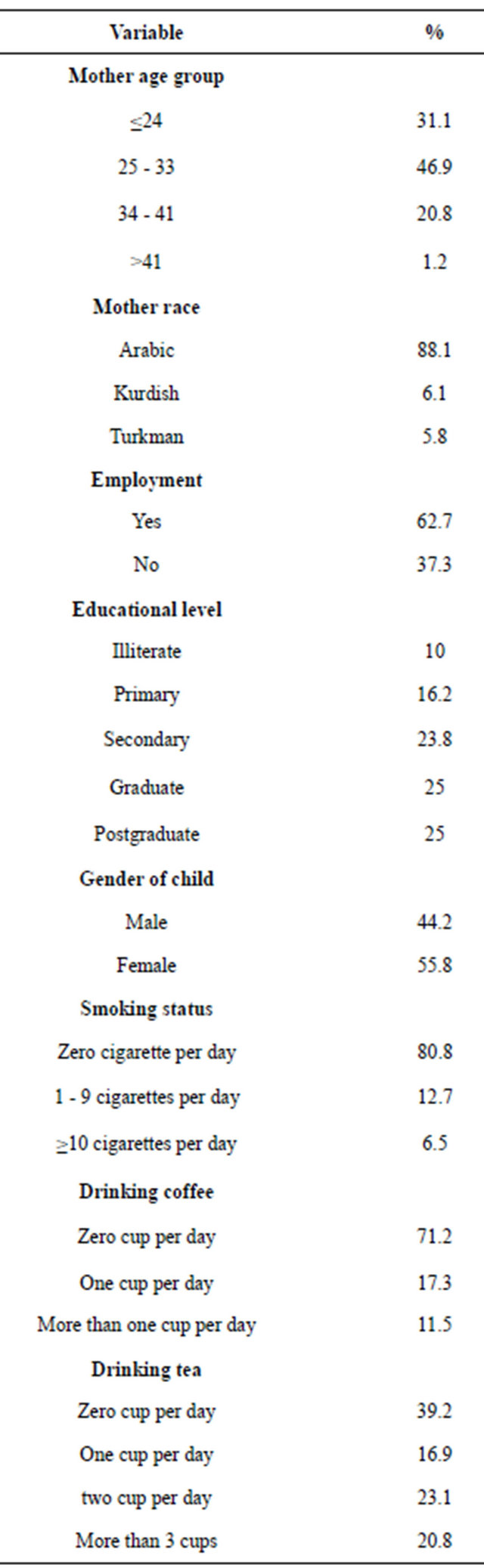
Table 2. Bivariate analyses of Sociodemographic, maternal life style and stress among cases and controls.
ing a child affected with ADHD. Exposure to other sociodemographic, and maternal life style risk factors like cigarette smoking and caffeine ingestion among mothers of cases and controls were identified.
Our study found a remarkable and independent 9 folds increased risk for ADHD associated with maternal exposure to war stress, giving a strong clue that maternal exposure to war stress was significantly associated with ADHD in the offspring (Adjusted OR 9.08, 95% CI 4.70 - 17.52, P < 0.001). This finding is consistent with most of the recent literature information about this correlation. It has also been shown that early postnatal stress in which the baby is already exposed to from the early months of pregnancy or even at later stage of pregnancy, predisposes the child to some serious developmental delays and
Table 3. Crude and adjusted odd ratios of significant variables.
behavioral problems [14].The current study supports the present literature which indicates that, exposure of the pregnant mother to stress exposes her foetus to the same sort of stress too [7].
Another study highlighted this association [15] who suggested that, especially during months 3 to 5 and 9 to 10 of pregnancy, maternal stress may increase the risk of the child for psychiatric disorders. These findings were similar with all previous studies which showed that child behavioral disturbance was directly related to maternal stress [16]. Although many studies have found a correlation between maternal stress and the subsequent development of ADHD symptoms in children [17] including this current study, but this association may not necessarily be a causal relationship. As ADHD is a very heritable disorder. It might be that, mothers who have experienced greater prenatal stress have a more significant history of ADHD themselves and confer greater genetic risk for ADHD to their offspring. Bearing in mind that our study did not investigate the genetic risk factor of developing ADHD, this would possibly constitute a limitation to our current study.
Another significant association in our study was an independent three-fold increased risk for ADHD associated with maternal exposure to nicotine smoking (Adjusted OR 3.27 95% CI 1.40 - 7.63 and P value < 0.001). In other words we can simply infer that, mothers who smoked during pregnancy were 3 times more susceptible to have children affected with ADHD. There is a controversy in the literature on this issue. One researcher [18] on twin siblings study found that, risk for ADHD was not significantly increased in subjects whose, mothers smoked during pregnancy.
Another researcher [19] however, found a positive association between smoking during pregnancy and ADHD in a big population-based sample. In one study [20] they have also found the same results.
On the other hand, there were many human studies which failed to find a significant link between maternal smoking during pregnancy and ADHD in the offspring. On contrary they found a protective association. One researcher [21] found a lower score on general cognitive functioning in 3-year-old children of mothers who smoked ≥ 10 cigarettes throughout pregnancy as compared with children whose mothers quit smoking just before pregnancy.
In spite of the findings of this current study of a significant association between maternal smoking and ADHD in the offspring, as well as some other similar findings in clinical studies, much more attention and caution should be paid before concluding that, those associations are causal relationships. One of the limitations of this study regarding the maternal smoking factor was that, only smoking status during pregnancy was investigated but the number and types of smoking were not included in this study.
Out of the other risk factors investigated in this study, we found an independent 2 fold increased risk for ADHD associated with one of the war stressors which is the damage of the family house and relocation. There was also an independent 3 fold increased risk for ADHD associated with another war stressor which is the loss of job for the father. Those stressors reflect the specific entity of the stress that most affected the pregnant mother. Stress in general was significant factor.
The last significant association in this study was the income of the family. The study found a significant association between the income of the family and ADHD (adjusted OR 1.02 95% 1.00 - 3.12, P < 0.001). The load of work pressure that the middle and high income families face may have a negative impact on their children. This fact may well explain the finding of this association.
This study did not explore data on genetic effects on offspring, or parental psychopathology or drug and alcohol abuse. Therefore, it is unwise to rule out the possibility that there are other unmeasured variables that might be associated with smoking or caffeine intake during pregnancy, which have in one way or another accounted for our findings. Another limitation was the recall bias in which mothers of cases may have provided qualitatively different information than mothers of controls. It is difficult to predict in which direction this bias would impact the current findings.
Mothers of children with ADHD might have been more keen to discover the main reason behind their children’s disorder, and could have inspired themselves more to remember the previous levels of exposure with very specific details. This may lead to inaccurate increase in odds ratio. On the other hand, mothers of ADHD children who have used substances during their pregnancy like nicotine or caffeine may feel guilty and therefore, try to underestimate their true levels of use more than mothers who have also used these substances during pregnancy but their children did luckily not suffer any illness or disorder. In this case the true odds ratio would have also been incorrectly decreased this time.
This study is one of the few studies that investigated the war effect on children. To our knowledge it’s the first study in Iraq investigating the association of war stress and ADHD. The place of the study is Baghdad (the Capital of Iraq) which is a big city with different, ethnic, national and religious backgrounds gives the study more strength and giving us more freedom to generalize our findings to all Iraq. Finally the multivariate logistic regression model used in the analyses of this study helped in adjusting and clearing the effects that may arise from effects of independent variables on each other’s and controlled for confounders.
On Post-traumatic stress among pregnant mothers, this study suggests psychosocial care in wars and disasters which involves:
1) Community self-help groups for emotional support and reestablishment of social connections;
2) Relaxation exercises for controlling and mastering physiological and psychological stress reactions, including hyper vigilance and avoidance;
3) Cultural metaphors and spiritual beliefs to facilitate cognitive processing and coming to terms with an overwhelming experience.
Protecting the pregnant mother and her baby from exposure to pollutants and toxins, including cigarette smoke, agricultural or industrial chemicals, is another recommendation that this study suggests in order to prevent ADHD occurrence in children.
Last but not least, this study aims to present policy makers a good benchmark for planning more programmes related to women and child health with respect to the fourth and fifth Millennium Development Goals (MDGs) for reduction of child mortality and morbidity and improvement of maternal health.
Attention deficit hyperactivity syndrome is a subject which draws attention of many scientists and physician worldwide due to the vague nature of the causes of it. The study which we did was a retrospective case-control study focusing on children with ADHD. It would be interesting in the future to follow a prospective cohort from conception to birth to latency age to examine how stress and other environmental factors would affect the development of various psychopathologies and how maternal stress influences the expression of selective symptoms in children who may be genetically predisposed to certain psychopathologies.
REFERENCES
- Faraone, S.V., Sergeant, J.A., Gillberg, C. and Biederman, J. (2003) The worldwide Prevalence of ADHD: Is it an American condition? World Psychiatry, 2, 104-113.
- Rohade, L.A., Beiderman, J., Busnello, E.A., et al. (1999) ADHD in a school sample of Brazilian Adolescents: A study of prevalence, comorbid conditions, and impairments. Journal of the American Academy of Child & Adolescent Psychiatry, 38, 716-722. doi:10.1097/00004583-199906000-00019
- Behrman, E. and Kleigman, M.J. (2004) Attention deficit hyperactivity disorder: Psychologic disorders. Nelson Textbook of Pediatrics, 3, 70-73.
- Biederman, J. and Faraone, S.V. (2005) Attention deficit hyperactivity disorder. Lancet, 48, 327-366.
- AlObaidi, A. and Ali, N.S. (2009) Attention deficit/hyperactivity disorder among schoolchildren in Baghdad. Journal of the American Academy of Child and Adolescent Psychiatry, 18, 4-5.
- Barkley, R.A., DuPaul, G.J. and McMurray, M.B. (1990) A comprehensive evaluation of attention deficit disorder with and without hyperactivity. Journal of Consulting and Clinical Psychology, 58, 775-789. doi:10.1037/0022-006X.58.6.775
- Teixeira, J.A.M., Fisk, N.M. and Glover, V. (1999) Association between maternal anxiety in pregnancy and increased uterine artery resistance index: Cohort based study. British Medical Journal, 318, 153-157. doi:10.1136/bmj.318.7177.153
- Modell, M., Mughal, Z. and Boyd, R. (1998) Brain development of the fetus: Neurological development of attention. Brain Development in Pediatrics, 6, 92-96.
- Rangon, C.M., Fortes, S., Lelièvre, V., Leroux, P., Plaisant, F., Joubert, C., Lanfumey, L., Cohen-Salmon, C. and Gressens, P. (2007) Chronic mild stress during gestation worsens neonatal brain lesions in mice. Journal of Neuroscience, 27, 7532-7540.
- Barrot, M., Marinelli, M., Abrous, D., Pont, F., Moal, M. and Piazza, P. (2001) The dopaminergic hyper-responsiveness of the shell of the nucleus accumbens is hormonedependent. European Journal of Neuroscience, 12, 973- 979. doi:10.1046/j.1460-9568.2000.00996.x
- Van den Berg, M.P. (2005) Prenatal psychopathology and the early developing child: The generation R study. European Journal of Neuroscience, 17, 55-58.
- Xu, X., Harville, E.W., Mattison, D.R., Elkind-Hirsch, K., Pridjian, G. and Buekens, P. (2011) Exposure to Hurricane Katrina, post-traumatic stress disorder and birth outcome: Errature. American Journal of Medical Sciences, 341, 85.
- Catani, C., Jacob, N., Schauer, E., et al. (2008) Family violence, war, and natural disasters: A study of the effect of extreme stress on children’s mental health in Sri Lanka. BMC Psychiatry, 8, 33. doi:10.1186/1471-244X-8-33
- Tol, W.A., Komproe, I.H., Susanty, D., et al. (2008) School-based mental health intervention for children affected by political violence in Indonesia: A cluster randomized trial. Journal of the American Medical Association, 300, 655-662. doi:10.1001/jama.300.6.655
- Wadhawa, P. (1998) Prenatal stress and life-span development. In: Friedman, H.S., Ed., Encyclopedia of Mental Health, Academic Press, San Diego, 265-280.
- Huttunen, M.O. and Niskanen, P. (1987) Prenatal loss of father and psychiatric disorders. Archives of General Psychiatry, 35, 429-431. doi:10.1001/archpsyc.1978.01770280039004
- Mash, E.J. and Johnston, C. (1990) Determinants of parenting stress: Illustrations from families of hyperactive children and families of physically abused children. Journal of Clinical Child Psychology, 19, 313-328. doi:10.1207/s15374424jccp1904_3
- Knopik, V.S., Sparrow, E.P., Madden, P.A., et al. (2005) Contributions of paternal alcoholism, prenatal substance exposure, and genetic transmission to child ADHD risk: A female twin study. Psychological Medicine, 35, 625-635. doi:10.1017/S0033291704004155
- Linnet, K.M., Wisborg, K., Obel, C., et al. (2005) Smoking during pregnancy and risk of hyperkinetic disorder in offspring. Pediatrics, 116, 462-467. doi:10.1542/peds.2004-2054
- Langley, K., Rice, F., Van den Bree, M.B. and Thapar, A. (2005) Maternal smoking during pregnancy as an environmental risk factor for attention deficit hyperactivity disorder behavior: A review. Minerva Pediatrica, 57, 359- 371.
- Sexton, M., Fox, N.L. and Hebel, J.R. (1990) Parental exposure to tobacco. Effects on cognitive functioning at age three. International Journal of Epidemiology, 19, 72- 77. doi:10.1093/ije/19.1.72