Health
Vol.5 No.8(2013), Article ID:35540,6 pages DOI:10.4236/health.2013.58175
Modifications of sexual activity during uncomplicated pregnancy: A prospective investigation of Spanish women
![]()
1Department of Obstetrics and Gynecology, San Cecilio University Hospital (HUSC), Granada, Spain; *Corresponding Author: raquelescuderorivas@hotmail.com
2Department of Obstetrics and Gynecology, University of Granada, Granada, Spain
Copyright © 2013 Raquel Escudero-Rivas et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received 23 May 2013; revised 1 July 2013; accepted 30 July 2013
Keywords: Sexuality; Frequency of Intercourse; Satisfaction; Orgasm
ABSTRACT
Introduction: Pregnancy is a time of profound changes in a woman’s life. These changes can influence her sexual behaviour and the relationship with her partner. The purpose of this article is to study sexual behaviour modification before and during pregnancy in a cohort of healthy Spanish pregnant women. Methods: This is a prospective cohort study in which 111 pregnant women took part. They completed a questionnaire about their sexual habits before pregnancy and at 20, 30 and 38 weeks (frequency of intercourse and orgasm, satisfaction with their relationships and pain or discomfort). Results: Intercourse frequency decreased progressively during pregnancy at all times studied relative to pre-pregnancy periods, to a significant degree (p < 0.0001), accompanied by a reduction in sexual satisfaction. The incidence of orgasm was lightly modified, except in the weeks before parturition in which it underwent a notable decrease (p < 0.0001) with an increase in the rate of hypoorgasmia/ anorgasmia from 19% pre-pregnancy to 43% at 38th week. Conclusions: The longitudinal monitoring of this cohort permits the conclusion that during pregnancy, sexual behaviour undergoes a general decline with respect to prepregnancy levels. The differences vary depending on the sexual parameter considered, with intercourse frequency being the most affected variable in contrast to dyspareunia, which is the least affected.
1. INTRODUCTION
Throughout a woman’s life, her sexual activity can undergo changes. The pregnancy and the puerperium are examples of this as they involve important physical and psychological changes for the woman in question, which can affect her sexuality and her relationship, impacting on desire, response and sexual behaviour [1-5].
Understanding the changes that occur in pregnancy is of prime importance since sexual dysfunctions can appear at this time, either because this is when they are initiated or because there are predisposing factors in pregnancy that become evident at this time [6-8].
Sexual response during pregnancy is very variable. Most authors agree that sexual activity and the frequency of intercourse and orgasm show a progressive reduction throughout pregnancy when compared to their extent prior to this [2,8-22]. The reduction of sexual desire may affect approximately 58% of pregnant women [14] and can even reach 72% depending on the study [15,20]. Alongside this, changes in certain activities that represent alternatives to intercourse such as masturbation, kisses, caresses, mammary stimulation, oral or anal sex have been described but these can vary from reductions [4,7,8,20,23] to persistence and increase [11-13]. Throughout pregnancy and postpartum the woman takes the initiative regarding sexual activity less frequently in contrast to those times previous to pregnancy [24].
This decline of sexual activity affects most pregnant women regardless of age, taking into account that younger women (under 20 years) maintain a higher level of sexual activity compared to a group of older women [16, 23,25-26]. These changes also seem to be observable in women with different parity with a notable reduction of intercourse frequency standing out in multiparous women during pregnancy in some studies [17,27], while others find that multiparous women have less orgasm problems compared to nulliparous women [28].
If these changes are analyzed by trimester, a light decrease in sexual interest is found during the first phase of pregnancy, followed by a variable pattern of behaviour in the final period of pregnancy [6,14,18,25] that can even approach levels defined as sexual dysfunction [29].
There are important differences in sexual response during pregnancy if socio-cultural and religious values are taken into account. For example, in contemporary Chinese societies traditional behaviours and beliefs persist, which involve women adopting a submissive and passive role in the relationship combined with a lack of information on sexual and reproductive issues. Due to this, there are still many women who abstain from maintaining sexual relations whilst pregnant [10,23,30]. Studies undertaken in Pakistani and Kuwaiti societies identify a significant reduction in sexual activity during pregnancy [3,31] especially in the last trimester. Adinma surveyed a group of Nigerian pregnant women and found a general reduction in sexual activity [9]. In many of these societies their remain fears and beliefs concerning the supposed negative effects of sexual relations on pregnancy and the foetus with intercourse seen to cause abortion, premature birth or damage to the foetus [3,9,20].
2. MATERIAL AND METHODS
An observational prospective cohort study was undertaken, in which involved 111 women who were attended by the Department of Obstetrics and Gynecology at San Cecilio University Hospital in Granada, Spain. Inclusion criteria used were that the women were healthy with uncomplicated pregnancies with low risk levels and with their pregnancies and parturition monitored and attended to at our hospital. The size of the study was determined by healthcare resources available in our hospital.
The participants were enrolled at their first obstetric visit at 12 weeks. They were informed verbally and by way of an informational leaflet about the objectives and nature of the study, as well as of the timing and mode of application of the surveys about their sexual activity. All of them signed to consent to their participation. We included only women who wanted to participate voluntarily in the study after receiving information about it.
Subsequently they were attended at 20 weeks of pregnancy (±1 week) and given the first questionnaire which sought information on their sexual habits prior to pregnancy and at 20 weeks. Subsequent questionnaires were completed at 30 weeks and shortly before birth (38 weeks). The number of questionnaires completed was 111 at 20 weeks, 106 at 30 weeks and 97 at 38 weeks. All of them had the same format. Firstly information on the frequency of sexual relations was collected with a choice of responses graded from lesser to greater frequency: infrequent (less than once a week), weekly (once a week), more than once a week or daily. Secondly they were asked about the incidence of orgasm during sex with a choice of answers ranging from rarely (never or occasionally), frequently or always. Thirdly the women answered questions about their satisfaction with their sexual relation (rejection/dissatisfaction, some satisfaction or general satisfaction). Finally they were asked about the presence of discomfort or pain in the sexual relation (never, sometimes, often/always).
The women included had to answer on an individual basis without the possibility of consulting with their partner and were also offered a private room to complete the questionnaire so that participants wouldn’t feel observed by the interviewer.
Responses were included as variables in the study in addition to the age, parity and other socio-economic and obstetric data not included in this study.
The data obtained were processed using the SPSS 17.0 statistical package. The Chi-squared test was employed for the analysis and comparison of the sexual activity variables; non-parametric methods such as the Wilcoxon and Friedman tests were used for paired samples.
3. RESULTS
A total of 111 pregnant women attended by our department participated in the study. The number of questionnaires completed were 111 in the prepregnancy, 111 at 20 weeks, 106 at 30 weeks and 97 at 38 weeks. The reasons for the loss of them were: ten preterm births (before 37 weeks), two cases of bleeding in the third trimester of pregnancy and two cases of preterm labor that forced sexual abstinence.
As shown in Table 1, the mean age was 30.3 years with 49.5% of the women under 30 and the remainder between 30 - 42 years (50.5%). The mean age of the first sexual relation was 19.3 years, in 30.6% of cases this was before 18 years and 53% between 18 - 22 years. Nulliparous women formed 55% of the total, 37.8% had had one child previously and 7.2% had had 2 or more children. Most of the women carried to term and only 9% had a premature birth (at less than 37 weeks).
If we analyze the frequency of intercourse before pregnancy and during it we find a progressive reduction in this variable (Table 2). Before pregnancy, infrequent (less than once a week) occurred in 9.9% of cases rising to 68% before parturition. In contrast, the incidence of the frequencies more than once a week and daily lessened considerably during pregnancy from 57.7% and 7.2% respectively to 13.4% and 2.1% at 38 weeks. There are significant statistical differences (p < 0.0001) between the frequency of intercourse before pregnancy and the three periods of pregnancy, which is evident as a progressive reduction. There are no differences between the
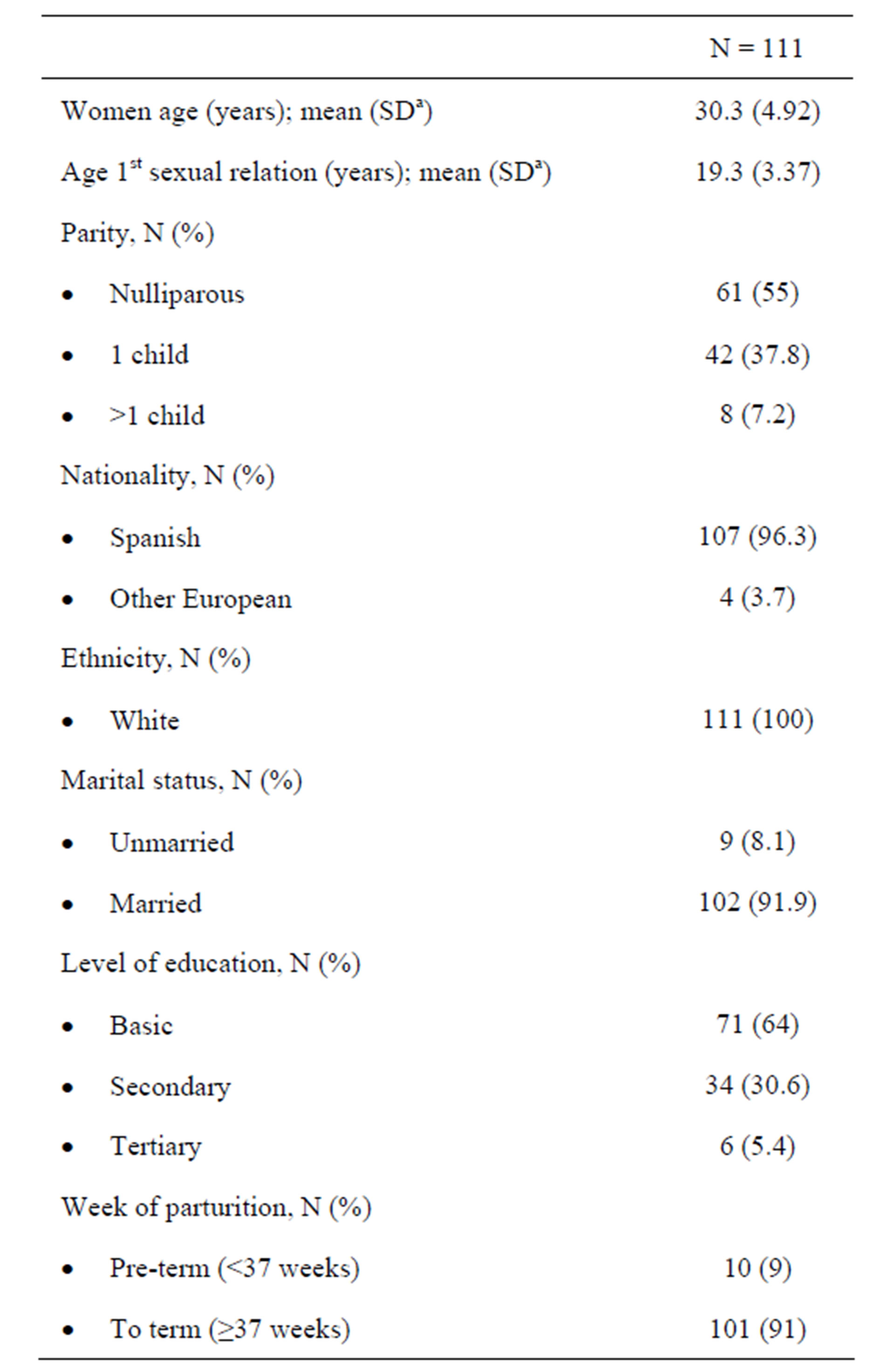
Table 1. Socio-demographic and obstetric characteristics of the pregnant women.
a. Standard deviation
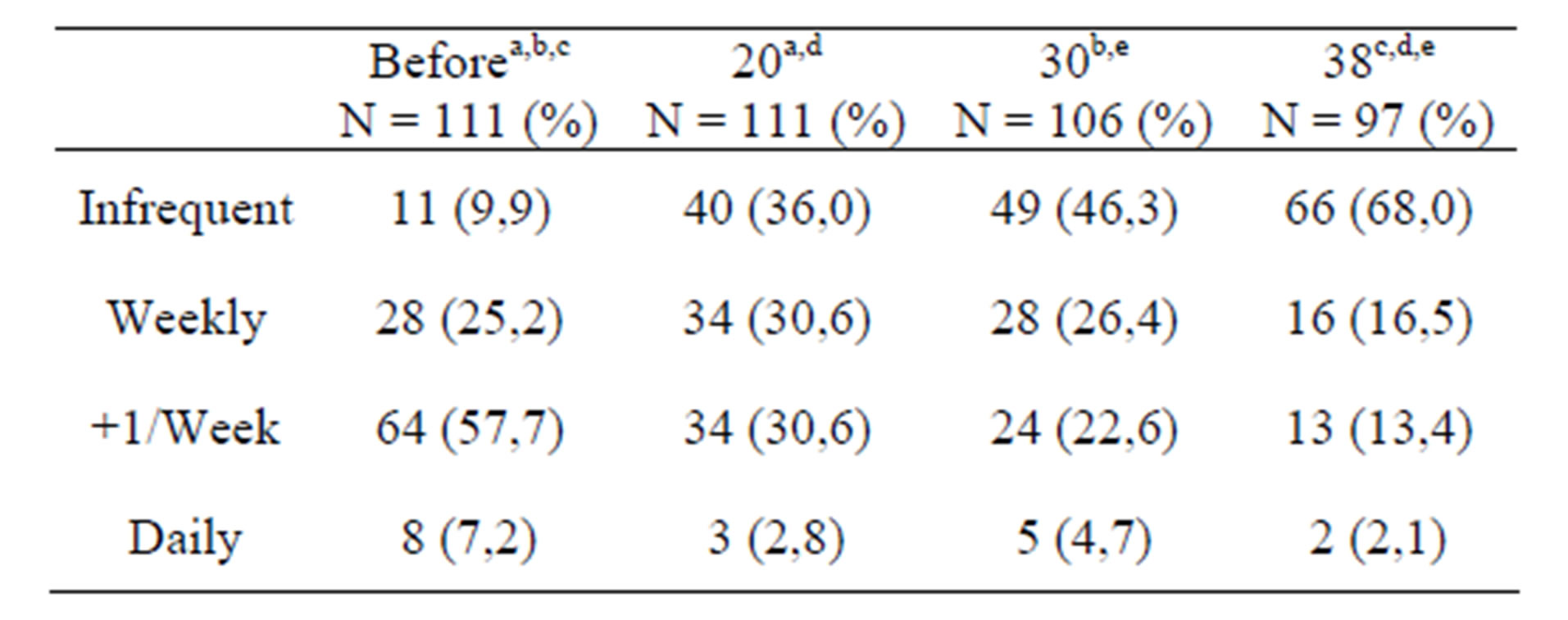
Table 2. Frequency of intercourse and week of pregnancy.
a,b,c,d,e: p < 0.0001 frequency of intercourse at 20 and 30 weeks but there are between these and the frequency at 38 weeks (p < 0.0001).
Likewise we analyzed the evolution of the frequency of orgasm finding an important reduction at 38 weeks (Table 3). The rate of anorgasmia/hypo-orgasmia (rare occurrence of orgasm) increases notably at 38 weeks with respect to the results previous to pregnancy (from 18.9% to 43.3%) with these differences being statistically significant, as well as those found between 38 weeks and 20 and 30 weeks (p < 0.001). However there is no significant difference between the pre-pregnancy data and the 20 and 30 weeks. Neither are significant the differences between the latter two.
With reference to satisfaction experienced in the sexual relation we found significant differences in satisfaction levels before pregnancy (p < 0.0001), at 20 weeks (p < 0.002) and at 30 weeks (p < 0.001) with respect to those at 38 weeks in the sense of a progressive decline (Table 4). Likewise there are notable differences between pre-pregnancy satisfaction levels and those found at 20 weeks (p < 0.003).
Finally, the incidence of pain or discomfort in the sexual relation before and during pregnancy didn’t present any statistically significant differences in any of the periods studied (Table 5). A greater incidence of habitual pain (often/always) stands out at 38 weeks (14.4%) respect to earlier levels (2.7%).
4. DISCUSSION
There have been many studies about sexual behaviour in pregnancy, although the number of prospective studies is limited. The importance of our study derives from the information collected about the sexual behaviour of the pregnant women in the period prior to pregnancy and during it, so that the evolution over time of sexuality in this cohort of healthy Spanish pregnant women can be analyzed.
The data obtained in our study confirm that the sexual function deteriorates during pregnancy as has been described by other authors [29,32].
The frequency of intercourse is a parameter that is altered considerably during pregnancy, being reduced pro-
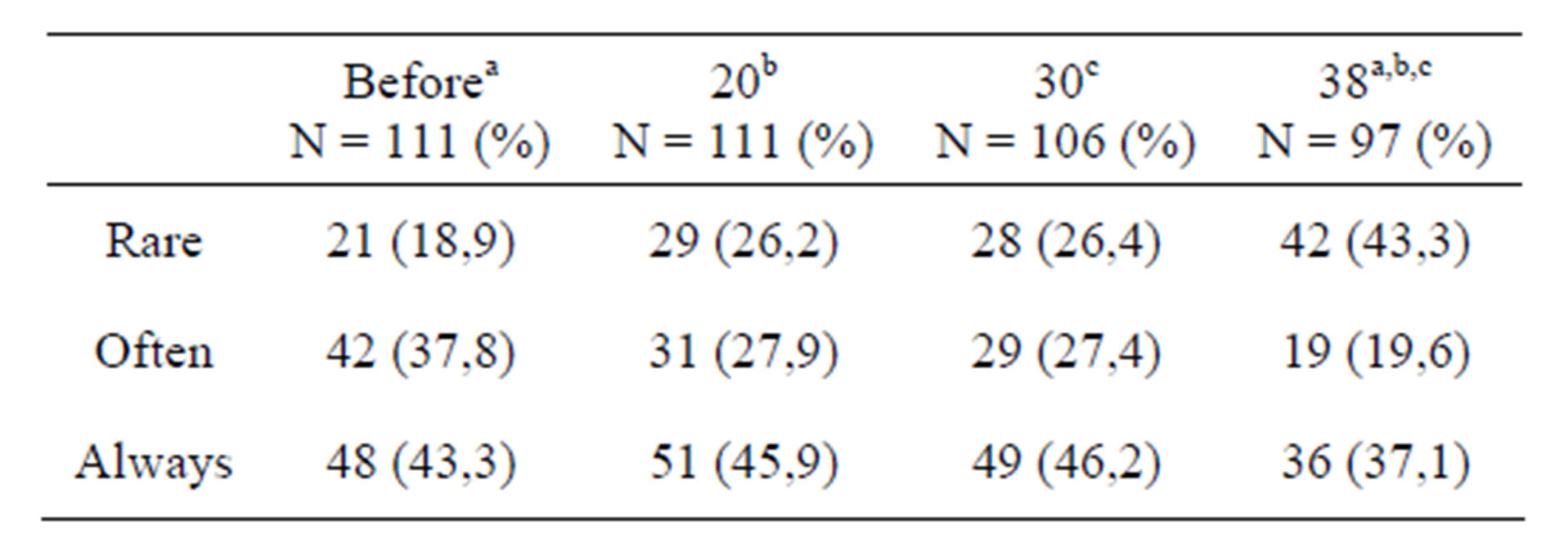
Table 3. Incidence of orgasm and week of pregnancy.
a: p < 0.0001. b y c: p < 0.001.
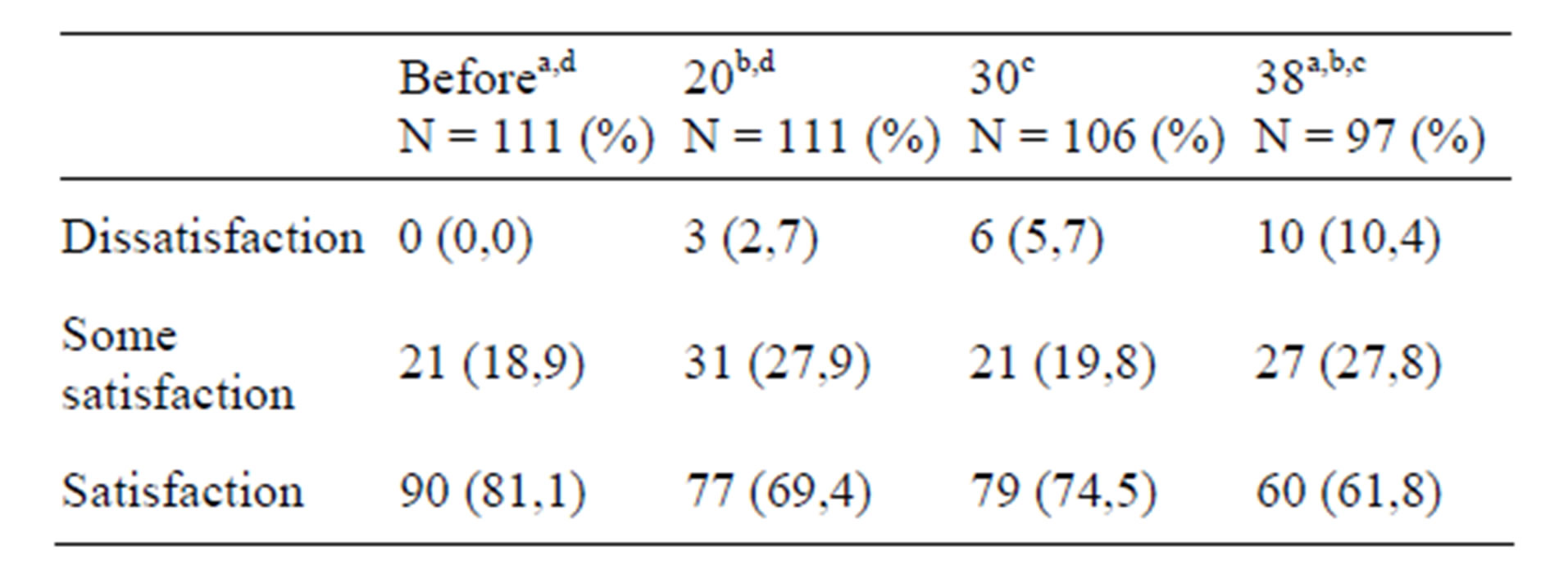
Table 4. Sexual satisfaction and week of pregnancy.
a: p < 0.0001. b: p < 0.002. c: p < 0.001. d: p < 0.003.
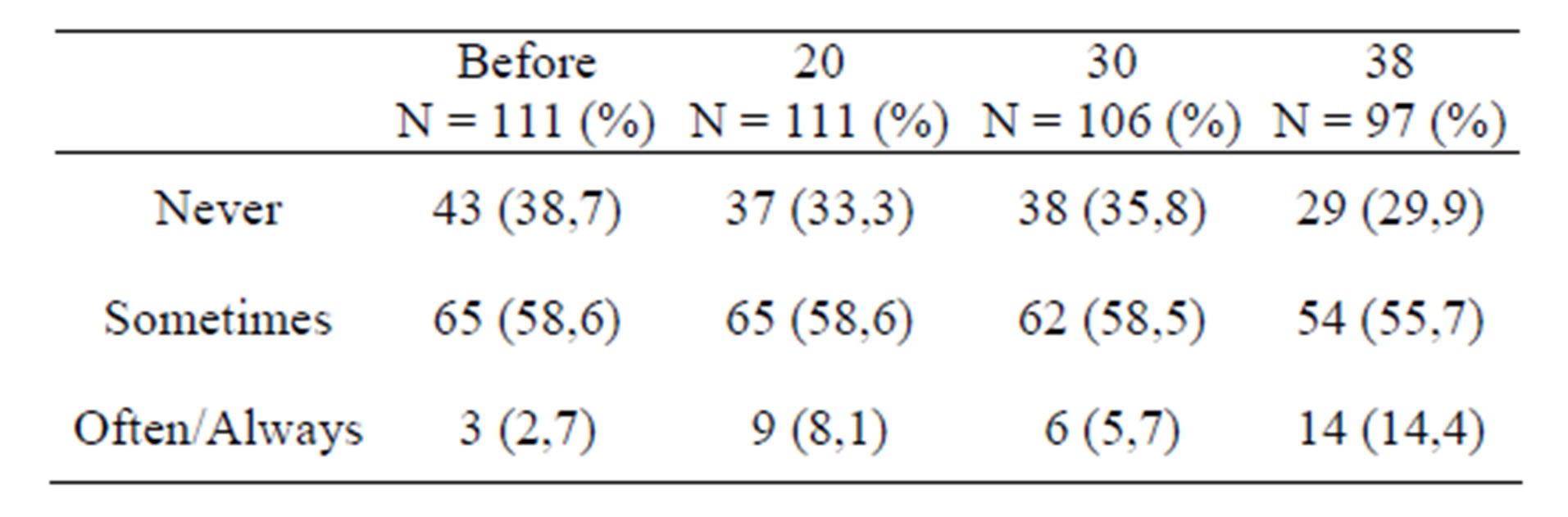
Table 5. Pain during intercourse and week of pregnancy.
gressively at all the times that were analyzed in the study relative to their pre-pregnancy values. In our study all of the pregnant women stated that they had maintained sexual relations before and during pregnancy although to varying degrees. In this way the low frequency of intercourse (less than once a week) underwent an important increase from 9.9% prior to pregnancy to 68% before parturition, whilst the frequency of more than once a week and daily prior to pregnancy reduced considerably from 57.7% and 7.2% respectively, compared to 13.4% and 2.1% at 38 weeks.
Hence an important reduction stands out in the frequency of intercourse in the first trimester, there is a less marked reduction between 20 and 30 weeks, with a further significant reduction in the period preceding parturition. These results are consistent with those found in other studies [8,14,20,23,33].
Nonetheless sexual behaviour can show a variable pattern during the second trimester of pregnancy with uneven results found in the literature [6,26]. In our study the frequency of intercourse reduced in this period although to a lesser degree than was the case in the first and third trimesters. On the other hand Bello [34] found that 91.7% of pregnant women maintained sexual relations during pregnancy with a notable rise in intercourse frequency in the second trimester, followed by a slight decrease at the end of pregnancy.
Most authors have noted a marked reduction of the sexual function in the final trimester [22,29,35-38]. This drop could originate from important physical changes pertaining to this period, such as the increase in abdominal volume and foetal weight or lumbar curvature. Other factors associated with the decline of the sexual function are tiredness, anxiety or fears of causing damage to the foetus or producing pregnancy complications [26].
Satisfaction levels during the sexual relation underwent similar variations to those found in the intercourse frequency although these were not so marked, remaining steadier during pregnancy. We observed a progressive decline throughout pregnancy as has been described by other authors [22,25,34].
In contrast to intercourse frequency the incidence of orgasm was only lightly affected during pregnancy except for the weeks leading up to parturition, in which was observed a reduction in the number of orgasms along with a significant increase in the incidence of anorgasmia/hypo-orgasmia from 18.9% before pregnancy to 43.3% at 38 weeks (p < 0.0001).
In our study all of the pregnant women had experienced orgasm prior to pregnancy. Only 2.8% of anorgasmia was found at 20 weeks, 5.7% at 30 weeks and 11.7% at 38 weeks.This contrasts with results from other studies in which the incidence of orgasm before pregnancy was present in 51% to 87% of cases [6,15]. For Connolly 87% of women experienced orgasm prior to pregnancy reducing progressively later on to drop to 33% in the third trimester [39].
Pauls undertook a prospective cohort study of pregnant women employing a series of validated questionnaires including the Female Sexual Function Index (FSFI), obtaining levels of sexual dysfunction in the third trimester with lower scores for the areas of orgasm and pain [29]. Erol applied the FSFI to 589 healthy pregnant women obtaining results showing that the most common symptoms of sexual dysfunction were reduction in clitoral sensitivity, lack of libido, followed by orgasmic dysfunction that affected 88% of the women in the third trimester [21].
We could surmise that this general decline in the sexual parameters, such as frequency or orgasmia, is due to the appearance of greater or lesser degrees of dyspareunia. In the literature we find that this symptom appears with variable frequency during pregnancy commonly affecting primiparous women [7,15] provoking a reduction in the number of sexual relations in pregnant women, more so in unmarried women than in married ones [40].
However our results don’t show that pregnancy involves a greater incidence of pain since the differences between periods of pregnancy were not significant, although we did find an increase in habitual pain (referred to as often/always) during intercourse in the third trimester relative to previous periods from 2.7% before pregnancy to 14.4% at the end of pregnancy.
The results obtained from our study indicate that dyspareunia increased as pregnancy progressed principally in the third trimester, as has been described by other authors [22,29,36]. On the contrary, Leite’s prospective cohort study of 271 healthy pregnant women described a reduction of dyspareunia during the third trimester in the two age groups included, both in younger women and in those over 20 years [26].
Our study presents some limitations. We did not use a validated questionnaire, although surveys were always the same in all obstetric visits: simple, easy and quick to answer. We included only women who wanted to participate voluntarily in the study after receiving information about it. Another limitation is that we asked pregnant women at 20 weeks about their sexuality at this time and before pregnancy.
As we have seen, pregnancy is a time of life in which there are multiple and profound changes that influence a woman’s sexual behaviour, generating a progressive deterioration of this in the majority of cases. The sexual history of each couple, the degree of satisfaction experienced by each individual with her own sexual activity, sexual health before pregnancy, the communication level within the relationship and especially the degree of information about the physiological changes that arise will all influence the manner in which the changes are dealt with, thereby determining whether or not there is a predisposition to suffer sexual disorders during pregnancy [8].
Pregnant women are often not informed of the most common changes at this time and they also encounter a lack of training and attention to these matters on the part of the healthcare workers that attend to them [20-23, 26,32,41,42]. For this reason a deeper understanding of changes in the sexual function during pregnancy is necessary alongside the diffusion among these professionals, so as to improve attention to pregnant women and their partners as well as their expectations during this period of their lives.
5. CONCLUSIONS
Our study described the variations in sexual activity in a cohort of healthy Spanish pregnant women during pregnancy to provide longitudinal monitoring and an evaluation of the evolution of this group in which there was a deterioration in sexual behaviour as a whole, although there were differences depending on the sexual parameter considered. The sexual parameter most affected during pregnancy was the frequency of intercourse. The presence of dyspareunia in pregnancy was the parameter of sexual behaviour least altered.
Once the pregnancy-related changes are described, it is evident that we must focus more deeply in future studies on which factors are related to the aforementioned changes.
REFERENCES
- White, S.E. and Reamy, K. (1982) Sexuality and pregnancy: A review. Archives of Sexual Behavior, 11, 429- 444. doi:10.1007/BF01541575
- Sueiro, E., Gayoso, P., Perdiz, C. and Doval, J.L. (1998) Sexuality and pregnancy. Atencion Primaria, 22, 340- 346.
- Naim, M. and Bhutto, E. (2000) Sexuality during pregnancy in Pakistani women. The Journal of the Pakistan Medical Association, 50, 38-44.
- von Sydow, K., Ullmeyer, M. and Happ, N. (2001) Sexual activity during pregnancy and after childbirth: Results from the Sexual Preferences Questionnaire. Journal of Psychosomatic Obstetrics and Gynecology, 22, 29-40. doi:10.3109/01674820109049948
- Glazener, C.M. (1997) Sexual function after childbirth: Women’s experiences, persistent morbidity and lack of professional recognition. British Journal of Obstetrics and Gynaecology, 104, 330-335. doi:10.1111/j.1471-0528.1997.tb11463.x
- von Sydow, K. (1999) Sexuality during pregnancy and after childbirth: A metacontent analysis of 59 studies. Journal of Psychosomatic Research, 47, 27-49. doi:10.1016/S0022-3999(98)00106-8
- Barrett, G., Pendry, E., Peacock, J., Victor, C., Thakar, R. and Manyonda, I. (2000) Women’s sexual health after childbirth. British Journal of Obstetrics and Gynaecology, 107, 186-195. doi:10.1111/j.1471-0528.2000.tb11689.x
- Pauleta, J.R., Pereira, N.M. and Graça, L.M. (2010) Sexuality during pregnancy. The Journal of Sexual Medicine, 7, 136-142. doi:10.1111/j.1743-6109.2009.01538.x
- Adinma, J.I. (1995) Sexuality in nigerian pregnant women: Perceptions and practice. Australian and New Zealand Journal of Obstetrics and Gynaecology, 35, 290-293. doi:10.1111/j.1479-828X.1995.tb01984.x
- Lee, J.T. (2002) The meaning of sexual satisfaction in pregnant taiwanese women. Journal of Midwifery and Women’s Health, 47, 278-286. doi:10.1016/S1526-9523(02)00264-7
- Solberg, D.A., Butler, J. and Wagner, N.N. (1973) Sexual behavior in pregnancy. The New England Journal Medicine, 288, 1098-1103. doi:10.1056/NEJM197305242882105
- Pepe, F., Pepe, P., Baldacchino, T., Laudani, L., La Greca, M. and Garozzo, G. (1989) Changes in the psychophysical experience of orgasm in pregnancy. Minerva Ginecologica, 41, 295-297.
- Perkins, R.P. (1982) Sexuality in pregnancy: What determines behavior? Obstetrics and Gynecology, 59, 189- 198.
- Bartellas, E., Crane, J.M., Daley, M., Bennett, K.A. and Hutchens, D. (2000) Sexuality and sexual activity in pregnancy. British Journal of Obstetrics and Gynaecology, 107, 964-968. doi:10.1111/j.1471-0528.2000.tb10397.x
- Ryding, E.L. (1984) Sexuality during and after pregnancy. Acta Obstetricia et Gynecologica Scandinavica, 63, 679- 682. doi:10.3109/00016348409154662
- Pepe, F., Panella, M., Pepe, P., Panella, P., Amaru, A. and Cantarella, M. (1988) Sexual behaviour in relation to age: A study of 205 puerperal woman. Clinical and Experimental Obstetrics and Gynecology, 15, 24-30.
- Pepe, F., Iachello, R., Panella, M., Pepe, G., Panella, P. and Pennisi, F. (1987) Parity and sexual behavior in pregnancy. Clinical and Experimental Obstetrics and Gynecology, 14, 60-56.
- Reamy, K., White, S.E., Daniell, W.C. and Le Vine, E.S. (1982) Sexuality and pregnancy. A prospective study. The Journal of Reproductive Medicine, 27, 321-327.
- Oruc, S., Esen, A., Lacin, S., Adiguzel, H., Uyar, Y. and Koyuncu, F. (1999) Sexual behaviour during pregnancy. Australian and New Zealand Journal of Obstetrics and Gynaecology, 39, 48-50. doi:10.1111/j.1479-828X.1999.tb03443.x
- Shojaa, M., Jouybari, L. and Sanagoo, A. (2009) The sexual activity during pregnancy among a group of Iranian women. Archives of Gynecology and Obstetrics, 279, 353- 356. doi:10.1007/s00404-008-0735-z
- Erol, B., Sanli, O., Korkmaz, D., Seyhan, A., Akman, T. and Kadioglu, A. (2007) A cross-sectional study of female sexual function and dysfunction during pregnancy. The Journal of Sexual Medicine, 4, 1381-1387. doi:10.1111/j.1743-6109.2007.00559.x
- Aslan, G., Aslan, D., Kizilyar, A., Ispahi, C. and Esen, A. (2005) A prospective analysis of sexual function during pregnancy. International Journal of Impotence Research, 17, 154-157. doi:10.1038/sj.ijir.3901288
- Fok, W.Y., Chan, L.Y. and Yuen, P.M. (2005) Sexual behavior and activity in Chinese pregnant women. Acta Obstetricia et Gynecologica Scandinavica, 84, 934-938.
- Sacomori, C. and Cardoso, F.L. (2010) Sexual initiative and intercourse behavior during pregnancy among brazilian women: A retrospective study. Journal of Sex and Marital Therapy, 36, 124-126. doi:10.1080/00926230903554503
- Bogren, L.Y. (1991) Changes in sexuality in women and men during pregnancy. Archives of Sexual Behavior, 20, 35-45. doi:10.1007/BF01543006
- Leite, A.P., Campos, A.A., Dias, A.R., Amed, A.M., De Souza, E. and Camano, L. (2009) Prevalence of sexual dysfunction during pregnancy. Revista da Associação Médica Brasileira, 55, 563-568. doi:10.1590/S0104-42302009000500020
- Adinma, J.I. (1996) Sexual activity during and after pregnancy. Advances in Contraception, 12, 53-61. doi:10.1007/BF01849546
- Witting, K., Santtila, P., Alanko, K., Harlaar, N., Jern, P. and Johansson, A. (2008) Female sexual function and its associations with number of children, pregnancy, and relationship satisfaction. Journal of Sex and Marital Therapy, 34, 89-106. doi:10.1080/00926230701636163
- Pauls, R.N., Occhino, J.A. and Dryfhout, V.L. (2008) Effects of pregnancy on female sexual function and body image: A prospective study. The Journal of Sexual Medicine, 5, 1915-1922. doi:10.1111/j.1743-6109.2008.00884.x
- Haines, C.J., Shan, Y.O., Kuen, C.L., Leung, D.H., Chung, T.K. and Chin, R. (1996) Sexual behavior in pregnancy among Hong Kong Chinese women. Journal of Psychosomatic Research, 40, 299-304. doi:10.1016/0022-3999(95)00644-3
- al Bustan, M.A., el Tomi, N.F., Faiwalla, M.F. and Manav, V. (1995) Maternal sexuality during pregnancy and after childbirth in Muslim Kuwaiti women. Archives of Sexual Behavior, 24, 207-215. doi:10.1007/BF01541581
- Serati, M., Salvatore, S., Siesto, G., Cattoni, E., Zanirato, M. and Khullar, V. (2010) Female sexual function during pregnancy and after childbirth. The Journal of Sexual Medicine, 7, 2782-2790. doi:10.1111/j.1743-6109.2010.01893.x
- Robson, K.M., Brant, H.A. and Kumar, R. (1981) Maternal sexuality during first pregnancy and after childbirth. British Journal of Obstetrics and Gynaecology, 88, 882- 889. doi:10.1111/j.1471-0528.1981.tb02223.x
- Bello, F.A., Olayemi, O., Aimakhu, C.O. and Adekunle, A.O. (2011) Effect of pregnancy and childbirth on sexuality of women in Ibadan, Nigeria. ISRN Obstetrics and Gynecology, 2011, 856586. doi:10.5402/2011/856586
- Eryilmaz, G., Ege, E. and Zincir, H. (2004) Factors affecting sexual life during pregnancy in eastern Turkey. Gynecologic and Obstetric Investigation, 57, 103-108. doi:10.1159/000075582
- Gökyildiz, S. and Beji, N.K. (2005) The effects of pregnancy on sexual life. Journal of Sex and Marital Therapy, 31, 201-215. doi:10.1080/00926230590513410
- DeJudicibus, M.A. and McCabe, M.P. (2002) Psychological factors and the sexuality of pregnant and postpartum women. Journal of Sex Research, 39, 94-103. doi:10.1080/00224490209552128
- Senkumwong, N., Chaovisitsaree, S., Rugpao, S., Chandrawongse, W. and Yanunto, S. (2006) The changes of sexuality in Thai women during pregnancy. Journal of the Medical Association of Thailand, 89, S124-S129.
- Connolly, A.M., Thorp, J. and Pahel, L. (2005) Effects of pregnancy and childbirth on postpartum sexual function: A longitudinal prospective study. International Urogynecology Journal, 16, 263-267. doi:10.1007/s00192-005-1293-6
- Steege, J.F. and Jelovsek, F.R. (1982) Sexual behavior during pregnancy. Obstetrics and Gynecology, 60, 163- 168.
- Sobecki, J.N., Curlin, F.A., Rasinski, K.A. and Lindau, S.T. (2012) What we don’t talk about when we don’t talk about sex: Results of a national survey of U.S. obstetriccian/gynecologists. The Journal of Sexual Medicine, 9, 1285-1294. doi:10.1111/j.1743-6109.2012.02702.x
- Johnson, C.E. (2011) Sexual health during pregnancy and the postpartum. The Journal of Sexual Medicine, 8, 1267- 1284. doi:10.1111/j.1743-6109.2011.02223.x