T. Ernstberger et al. / J. Biomedical Science and Engineering 3 (2010) 181-186
Copyright © 2010 SciRes.
186
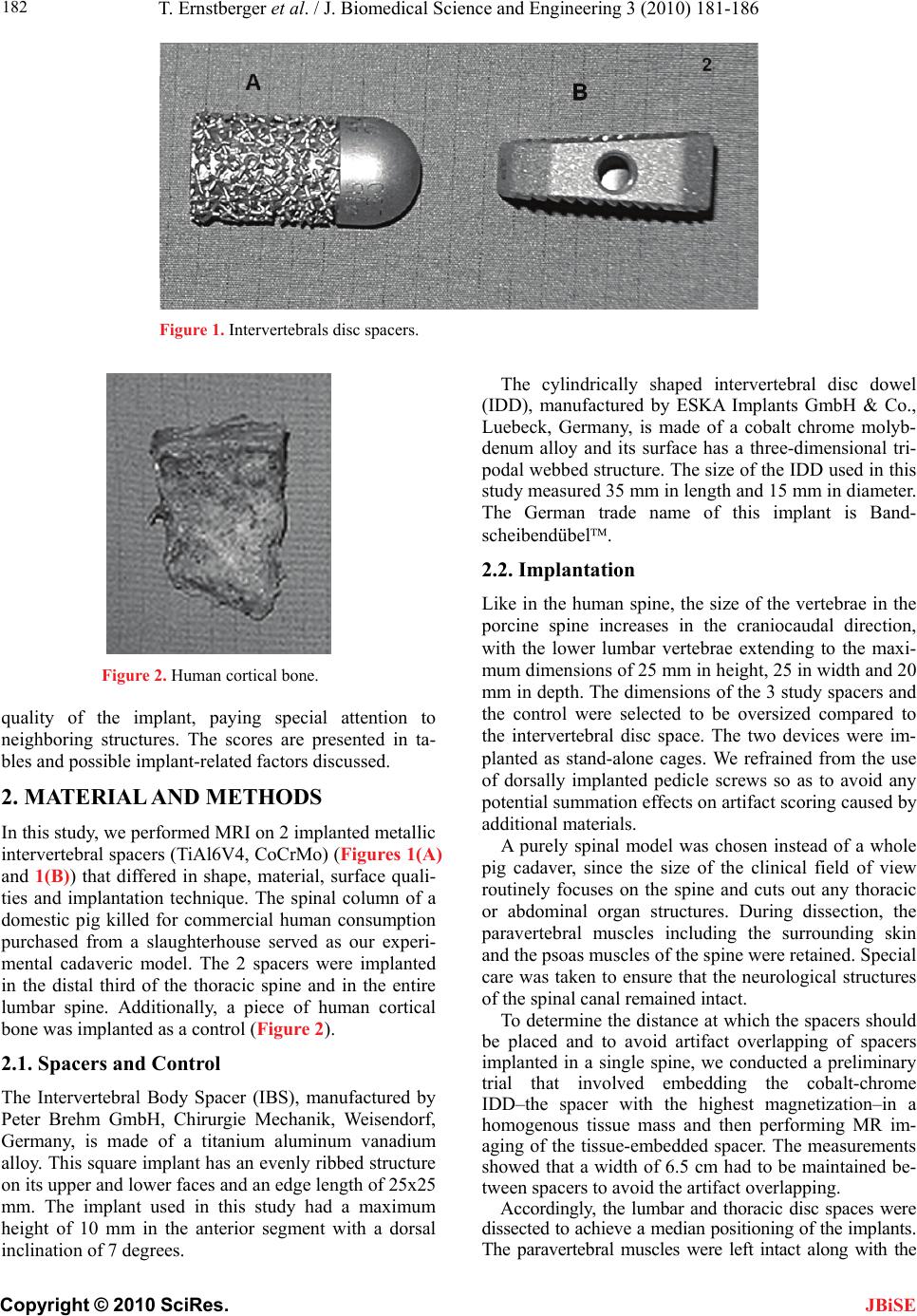
tebral spacer
m
s of the intervertebral spacers
spine fusion cause susceptibil-
., Parizel, P.M. and Jinkins, J.R. (2002)
RI of the postoperative lumbar s
rative study of MR imaging profile of titanium
rs, B.N. and Eisenstein, S.M. (1989) Donor site
) A carbon fiber
. and
eduction
mpp, S., Breitenseher, M.,
, Ebraheim, N.A., Savolaine, E.R. and Jackson,
, Lewin, J.S., Duerk, J.L., Yoo, J.U. and
hew, J.T. and
, A.R., Chesnut, R.M., Scuderi, G., Healy, J.F.,
neider, U., Breusch, S.J., Hansmann, J.
In another cadaveric artifact study, Wang et al. [18]
described the MRI behavior of an interver
JBiSE
ade of titanium. Using T1 SE sequences, the implant-
related artifact rate of the titanium spacer was primarily
limited to the implant’s direct surroundings and anat-
omic neighboring structures were clearly distinguisha-
bility. In our study, when T1 TSE sequences were used
to image both metallic spacers, neither implant shape nor
implant position could be distinguished with certainty. In
a phantom study by Rudisch et al. [16], the relevance of
metallic artifacts and implant-related characteristics,
such as implant material, shape and position, was dem-
onstrated in addition to an impact by the selected MRI
sequence. In spite of the use of optimum MRI sequences,
variability in the amount of susceptibility artifacts must
be accounted for when evaluating MRI scans of metallic
spine implants.
6. CONCLUSIONS
of a
The designs and material
currently used in anterior
ity artifacts that can be rated by validated scoring sys-
tems. Of 15 sequences tested, T1 TSE sequences pro-
duced the best spacer imaging for both metallic implants
tested. An interobserver-validated scoring system proved
effective in ranking the relevance of spacer material on
MRI imaging quality. Studies are ongoing to further de-
velop MRI scoring systems and establish optimum im-
aging sequences for post-fusion diagnostics.
REFERENCES
[1] Van Goethem, J.W
Review article: Mpine. Massie, J.B. and Garfin, S.R. (1994) Metallic spinal arti-
facts in magnetic resonance imaging. Spine, 19, 1237-42.
[16] Rudisch, A., Kremser, C., Peer, S., Kathrein, A., Judmaier,
Neuroradiology, 44, 723-39.
[2] Herold, T., Caro, W.C., Heers, G., Perlick, L., Grifka, J.,
Feuerbach, S., Nitz, W. and Lenhart, M. (2004) Influence
of sequence type on the extent of the susceptibility arti-
fact in MRI: A shoulder specimen study after suture an-
chor repair. Rofo, 176, 1296-301.
[3] Schenck, J.F. (1996) The role of magnetic susceptibility
in magnetic resonance imaging: MRI magnetic compati-
bility of the first and second kinds. Med Phys, 23,
815-50.
[4] Malik, A.S., Boyko, O., Atkar, N. and Young, W.F. (2001)
A compa mart
pedicle screws. Acta Radiol, 42, 291-3.
[5] Goulet, J.A., Senunas, L.E., DeSilva, G.L. and Greenfield,
M.L. (1997) Autogenous iliac crest bone graft: Compli-
cations and functional assessment. Clin Orthop, 339,
76-81.
[6] Summe
pain from the ilium: A complication of lumbar spine fu-
sion. J Bone Joint Surg Br, 71, 677-80.
[7] Brantigan, J.W. and Steffee, A.D. (1993
implant to aid interbody lumbar fusion: Two-year clinical
results in the first 26 patients. Spine, 18, 2106-7.
[8] Fellner, C., Behr, M., Fellner, F., Held, P., Handel, G
Feuerbach, S. (1997) Artifacts in MR imaging of the
temporomandibular joint caused by dental alloys: A
phantom model study at T1.5. Rofo, 166, 421-8.
[9] Fritzsche, S., Thull, R. and Haase, A. (1994) R
rtifacts in magnetic resonance images by using opti-
mized materials for diagnostic devices and implants.
Biomed Tech (Berl), 39, 42-6.
[10] Henk, C.B., Brodner, W., Gra
Thurnher, M., Mostbeck, G.H. and Imhof, H. (1999) The
postoperative spine. Top Magn Reson Imaging, 10,
247-64.
[11] Rupp, R.
W.T. (1993) Magnetic resonance imaging evaluation of
the spine with metal implants: General safety and supe-
rior imaging with titanium. Spine, 18, 379-85.
[12] Ortiz, O., Pait, T.G., McAllister, P. and Sauter, K. (1996)
Postoperative magnetic resonance imaging with titanium
implants of the thoracic and lumbar spine. Neurosurgery,
38, 741-5.
[13] Petersilge, C.A.
Ghaneyem, A.J. (1996) Optimizing imaging parameters
for MR evaluation of the spine with titanium pedicle
screws. AJR Am J Roentenol, 166, 1213-8.
[14] Wang, J.C., Sandhu, H.S., Yu, W.D., Minc
Delamarter, R.B. (1997) MR parameters for imaging ti-
tanium spinal instrumentation. J Spinal Disord, 10,
27-32.
[15] Vaccaro
W. and Daniaux, H. (1998) Metallic artifacts in magnetic
resonance imaging of patients with spinal fusion: A
comparison of implant materials and implant sequences.
Spine, 23, 692-9.
[17] Thomsen, M., Sch
and Freund, M. (2001) Artifacts and ferromagnetism de-
pendent on different metal alloys in magnetic resonance
imaging: An experimental study. Orthopade, 30, 540-4.
[18] Wang, J.C., Yu, W.D., Sandhu, H.S., Tam, V. and Dela-
er, R.B. (1998) A comparison of magnetic resonance
and computed tomographic image quality after the im-
plantation of tantalum and titanium spinal instrumenta-
tion. Spine, 23, 1684-8.