World Journal of Cardiovascular Surgery
Vol.3 No.2(2013), Article ID:33408,3 pages DOI:10.4236/wjcs.2013.32015
A Surgical Case of Primary Cardiac Osteosarcoma Arising from Mitral Posterior Leaflet
1Department of Cardiovascular Surgery, Cardiovascular Center, Kyoto-Katsura Hospital, Kyoto, Japan
2Department of Internal Medicine, Minami Osaka General Hospital, Osaka, Japan
3Department of Thoracic and Cardiovascular Surgery, Minami Osaka General Hospital, Osaka, Japan
4Department of Pathology, Minami Osaka General Hospital, Osaka, Japan
Email: *mmorita@ katura-cvs-com
Copyright © 2013 Masafumi Morita et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received February 26, 2013; revised March 26, 2013; accepted April 3, 2013
Keywords: Cardiac Tumor; Surgery; Osteosarcoma; Mitral Valve
ABSTRACT
Little is reported about primary cardiac osteosarcoma from mitral valve. We report a surgical case of primary cardiac osteosarcoma arising from mitral valve. The patient was a 54-year-old woman with congestive heart failure caused by mitral regurgitation due to a tumor (30 × 20 mm) from the posterior leaflet. We performed complete resection of the tumor combined with the mitral valve and replaced it to a mechanical valve. Histopathological examination showed evidence of complete excision of cardiac osteosarcoma. Sixteen months after the initial surgery, the mechanical valve has a trouble with its opening of leaflets due to local recurrence in the mitral annulus, and 2nd mitral valve replacement following tumor excision was performed. Eighteen months after the 2nd surgery, the patient finally died by recurrence as well as invasion of osteosarcoma from mitral annulus to left ventricular myocardium. We discussed about the management and treatments of primary cardiac osteosarcoma in this case.
1. Introduction
Primary osteosarcoma of the heart is rare. In the patients with primary cardiac sarcoma, complete surgical resection of the tumor is recognized as the most effective and essential treatment to obtain longer survival period for the patients [1]. In this case, we accomplished complete surgical resection and mitral valve replacement (MVR) against primary cardiac osteosarcoma arising from mitral posterior leaflet. Despite the complete resection of the primary tumor, the local recurrence caused the prosthetic valve dysfunction leading to severe congestive heart failure. Although there are some case reports of primary cardiac sarcoma from left and right atrial wall, little is reported about primary cardiac sarcoma from mitral valve [2]. In this report, we discussed about the management and treatments of primary cardiac osteosarcoma from mitral valve.
2. Clinical Summary
A previously healthy 54-year-old woman was transferred to our hospital because of the gradual development of dyspnea as well as shortness of breath after light exercise. Her symptoms had begun one month prior to visiting our hospital. On physical examination, a systolic heart murmur of Levine III/VI was audible at the apex. Laboratory data were within normal range. Chest radiography revealed bilateral pulmonary congestion and right pleural effusion. Transthoracic echocardiography demonstrated an abnormal mass, which appeared to be a partially calcified myxomatous tumor or vegetation, located in the posterior leaflet of mitral valve (Figure 1).
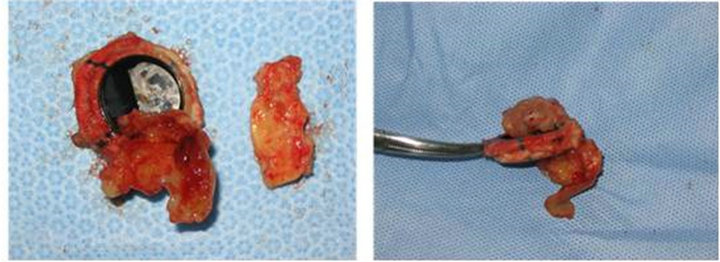
After general evaluation, we made a decision of a surgical resection of the tumor. Following median sternotomy, total cardiopulmonary bypass was established by bicaval venous drainage and ascending aortic arterial return. The ascending aorta was cross-clamped, and coldpotassium cardioplegia was given in antegrade fashion. We selected trans-septal approach to reach the tumor. The tumor arose from mitral posterior leaflet. We resected the tumor combined with the posterior leaflet, and performed MVR using ATS 25 mm prosthetic valve. The excised tumor size was 30 × 20 × 15 mm and weighed 5.1 g (Figure 2(a)). Histopathological examination demonstrated cardiac osteosarcoma (Figure 2(b)). The postoperative course was uneventful.
Sixteen months after the initial surgery, she complained dyspnea, and noticed lack of closing sound of the prosthetic valve. Ultrasound echocardiography and chest radiography showed congestive heart failure as well as dysfunction of the mitral prosthetic valve due to local recurrence of the tumor. In order to improve function of the prosthetic valve, we used the same approach as the 1st surgery to reach the mitral valve. As shown in Figures 3(a) and (b), the recurrence of osteosarcoma locally developed climbing over a part of sewing cuff of the prosthetic valve resulting in interference of opening of the prosthetic valve. We resected the growing tumor combined with the prosthetic valve. Tissue of the mitral annuls in which the tumor developed was hard. These operative findings indicated the local recurrence of cardiac osteosarcoma. We performed 2nd MVR. The postoperative course was uneventful.
One year later, the patient was admitted to our hospital
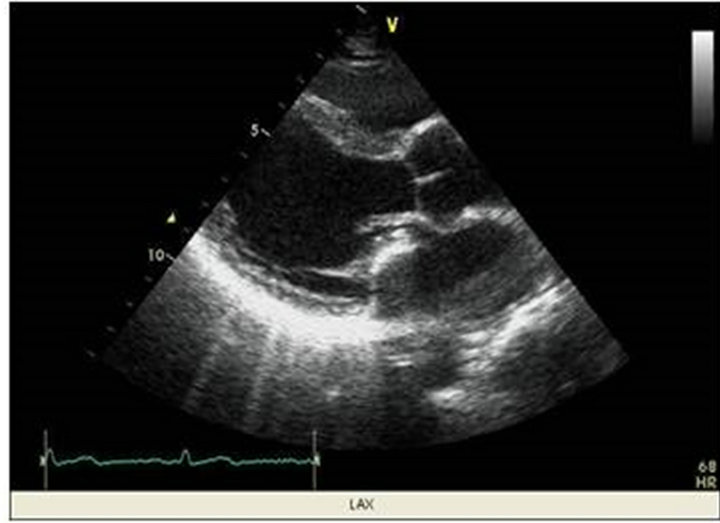
Figure 1. Ultrasound echocardiography demonstrated a tumor including high echoic region located in mitral posterior leaflet.
 (a) (b)
(a) (b)
Figure 2. (a) The tumor was completely resected with posterior leaflet of mitral valve. Arrows indicated the posterior leaflet of mitral valve; (b) The picture demonstrated typical histopathological findings of osteosarcoma including a number of growing spindle shaped cells and osteoid formation (right upper corner) in the resected tumor.
 (a) (b)
(a) (b)
Figure 3. The picture of 2nd surgery due to mechanical valve dysfunction by local recurrence of cardiac osteosarcoma. (a) The picture showed the local recurrence of cardiac osteosarcoma resulting in dysfunction of the prosthetic valve; (b) The picture of the lateral view presented the local recurrence of cardiac osteosarcoma expanding from mitral annulus to left atrium as well as left ventricle.
by severe congestive heart failure combined with bilateral pleural effusion due to the prosthetic valve dysfunction again. In order to regain the prosthetic valve function, we performed the 3rd operation. According to the operative findings, the growing tumor expanded and occupied for 2/3 of the space in left atrium, and invaded from the mitral annulus extended to the left ventricle. We resected the tumor as much as possible, and replaced the prosthetic valve. Tracheostomy was required because of prolonged ventilation and respiratory instability. Finally, 6 months after the 3rd MVR, the patient died due to dissemination of osteosarcoma expanding into left atrium and ventricle.
3. Discussion
Primary sarcomas of the heart are rare. Recent publications by retrospective studies report about each 30 cases collected during 20 - 30 years from multiple medical centers in the United States of America [1,2]. In terms of tumor location, more than 80% arise in atrium and pulmonary vessels. Pathologically, angiosarcoma is the most common type (about 50%) in the cardiac sarcomas. In these reports, cardiac sarcomas diagnosed as osteosarcoma as well as originated from mitral valve are only present in 3.7% (1/27) and 6.9% (2/29), respectively[1,2]. As shown in our case, little is reported about primary cardiac osteosarcomas arising from mitral valve.
Complete surgical resection is essential to obtain longer survival in the patients with primary cardiac sarcoma. Bakaeen and colleagues et al reported that local recurrence of cardiac sarcomas occur in a group (R1) in which sarcoma cells are microscopically positive in the surgical margin, not in R0 group [1]. In this case, we completely resected the tumors combined with mitral valve. However, 16 months after the initial surgery, dysfunction of the prosthetic valve was caused by local recurrence of cardiac osteosarcoma. These clinical findings indicated that sarcoma cells far from mitral valves might independently exist around the mitral annulus. Even though tumor is surgically resected, the extended surgery such as autotransplant [3] occasionally may be required to achieve complete surgical resection of the cardiac sarcomas at the initial surgery. Furthermore, as shown in this case, local recurrence of cardiac sarcoma from mitral valve and/or annulus resulted in dysfunction of the prosthetic valve. Considering the way of the tumor growth of cardiac sarcoma, it is difficult to distinguish the real margin of the primary tumor without microscopic evaluation. In addition, following the complete resection of the tumor, cardiac reconstruction may be technically challenging.
It is generally accepted that the prognosis of cariac osteosarcoma is poor. A median survival period is 23.5 months after surgical resection with curative intent [1]. In this case, the survival period was 34 months after the initial surgery, although repetitive MVR was needed by the prosthetic valve dysfunction due to local recurrence of osteosarcoma. The results in this case were acceptable compared with the previous reports. Adjuvant chemotherapy and/or radiation therapy are considered for additional options in combination with the complete tumor resection. However, the effectiveness for prognosis remains obscure.
In this case we experienced a rare case of primary cardiac osteosarcoma arising from mitral posterior leaflet, and performed MVR after the complete surgical resection of the tumor. In patients with primary cardiac sarcoma from mitral valve, the local recurrence was directly associated with dysfunction of the mitral prosthetic valve. In the follow-up period, careful attention should be taken for the prosthetic valve dysfunction as well as congestive heart failure suggesting the local recurrence and/or invasion.
REFERENCES
- F. G. Bakaeen, D. E. Jaroszewski, D. C. Rice, et al., “Outcomes after Surgical Resection of Cardiac Sarcoma in the Multimodality Treatment Era,” The Journal of Thoracic and Cardiovascular Surgery, Vol. 137, No. 6, 2009, pp. 1454-1460. doi:10.1016/j.jtcvs.2008.11.026
- P. J. Zhang, J. S. Brooks, J. R. Goldblum, et al., “Primary Cardiac Sarcomas: A Clinicopathologic Analysis of a Series with Follow-Up Information in 17 Patients and Emphasis on Long-Term Survival,” Human Pathology, Vol. 39, No. 9, 2008, pp. 1385-1395. doi:10.1016/j.humpath.2008.01.019
- M. J. Reardon, C. A. DeFelice, R. Sheinbaum, et al., “Cardiac Autotransplant for Surgical Treatment of a Malignant Neoplasm,” The Annals of Thoracic Surgery, Vol. 67, No. 6, 1999, pp. 1793-1795. doi:10.1016/S0003-4975(99)00343-4
NOTES
*Corresponding author.