Open Journal of Preventive Medicine
Vol.2 No.1(2012), Article ID:17414,7 pages DOI:10.4236/ojpm.2012.21011
What is the role of adolescent body mass index and physical activity on adult health risk behaviors?
![]()
1Department of Human Performance and Exercise Science, Youngstown State University, Youngstown, USA; *Corresponding Author: japintar@ysu.edu
2Department of Epidemiology, University of Pittsburgh, Pittsburgh, USA
3Department of Biostatistics, University of Pittsburgh, Pittsburgh, USA
4Department of Health and Physical Activity, University of Pittsburgh, Pittsburgh, USA
Received 11 October 2011; revised 21 November 2011; accepted 22 December 2011
Keywords: Smoking; Drinking; Binge Drinking
ABSTRACT
Introduction: A high prevalence of modifiable risk factors exists among adolescents that may lead to increased levels of morbidity and mortality in adulthood. This study sought to determine whether higher levels of physical activity (PA) and/or having a healthy body weight in adolescence influences future health risk behaviors (HRB) in young adulthood. Methods: Complete data were gathered for 536 participants from a prospective study and a follow-up survey conducted 10 years apart. At both time points, the questionnaires included information about HRB, PA, and health status. Results: Males who engaged in HRB during adolescence were more likely to continue these same risk behaviors during adulthood. Using multivariate models, only HRB in adolescence predicted HRB in adulthood for drinking, binge drinking and smoking among males, and for binge drinking and smoking among females. Conclusions: It appears that for males, once a health-risk behavior is initiated, it will likely continue into young adulthood, regardless of the presence of other healthy behaviors such as the proper maintenance of body weight and higher levels of PA. Similarly for females, binge drinking and smoking in adolescence is predictive of the same behavior in adulthood.
1. INTRODUCTION
According to the CDC, modifiable risk factors such as smoking, alcohol consumption, physical inactivity and poor diet are leading causes of morbidity and mortality in the United States [1]. National survey data [2] indicate a high prevalence of these modifiable risk factors among adolescents. It is thought that the adolescent years are a period during which adult health behaviors begin to develop [3]. For this reason, many public health initiatives identify childhood as a critical time for promoting healthy behaviors such as adequate physical activity levels and maintenance of a healthy body weight. However, a link between increased physical activity levels and the maintenance of a healthy weight in adolescence with less risk taking behaviors in young adulthood has not been established.
The risk taking behaviors of interest in the present investigation focus on alcohol use and smoking. As a student progresses from middle school to high school, the likelihood of drinking alcohol, binge drinking and/or smoking increases, while the percentage of those maintaining an appropriate body weight and adequate physical activity level decreases [4,5]. Reports from the Youth Risk Behavior Surveillance System (YRBSS) and Behavioral Risk Factor Surveillance System (BRFSS) indicate that the percentage of adolescents who report consuming at least one drink of alcohol during the previous month increases dramatically from 7% of 12 - 14 years old to 27.5% of 15 - 17 years old [4,5]. This percentage continues to rise in the 18 - 20 years old category with values approximating drinking percentages during adulthood (51.3% and 54.3%, respectively). Similarly, binge drinking, defined as consuming five or more alcoholic drinks on at least one occasion in the past 30 days, also appears to peak between the ages of 18 - 20 years with 36.3% reporting the behavior. The second highest percent of binge drinkers are the 15 - 17 years old (17.8%), followed by adults (15.7%) and then those aged 12 - 14 years (3.3%) [4,5]. When examining this trend by gender, underage males were more likely than underage females to be current alcohol users (29.4% vs 27.8%, respectively) and binge drinkers (21.6% males, 16.5% females). Smoking has also been shown to increase throughout the high school years. According to the 2009 YRBSS, smoking prevalence increased from 13.5% in ninth grade to 18.3% in tenth, 22.3% in eleventh grade and peaked at 25.2% in twelfth grade [4]. The prevalence of smoking decreases in adulthood with 17.9% of adults classified as current smokers [5].
In regard to health status, physical activity tended to decrease during the same time frame of ninth to twelfth grade. The percentage of students not participating in 60 minutes of physical activity on any of the seven days prior to the survey, increased from 21.8% in 9th grade, 22.6% in tenth, 22.9% in eleventh to 25.6% in twelfth [4]. In addition, the percent of students who were classified as either overweight or obese was highest in ninth grade (29.0%), dropped slightly during tenth (27.9%) and eleventh (25.8%) grades and increased again during twelfth grade (28.2%) [4,5].
When examining whether risk-taking behaviors during adolescence impact young adulthood behaviors, both alcohol use [6-8] and cigarette smoking [9] have been suggested as factors that may predict future obesity. These predictions of future obesity have been questioned by other researchers as to whether weight gain in young adulthood is mediated more so by factors typically associated with alcohol consumption and smoking such as overeating and physical inactivity [10,11]. To date, no studies have examined whether being overweight/obese or having an inadequate physical activity level during adolescence predicts future alcohol or cigarette use during young adulthood. It is hypothesized that maintaining an appropriate weight and activity level during adolescence may prevent future risk-taking behaviors such as excessive alcohol use and cigarette smoking in adulthood. It has been suggested that physical activity is an alternative, competing, and pleasurable behavior, which may provide mood benefits and function as a coping skill in some high-risk situations for relapse [12-14]. Therefore, the purpose of this study was to determine whether higher levels of physical activity and/or maintenance of a healthy body weight in adolescence influences future risk taking behaviors such as smoking and drinking alcohol in young adulthood. Specifically, it is believed that adolescents who maintain an active lifestyle and healthy body weight throughout middle to high school years will be less likely to engage in the risk taking behaviors of drinking, binge drinking and smoking during young adulthood.
2. METHODS
2.1. Study Population
Study subjects for this investigation come from the Epidemiology of Physical Activity from Adolescence to Adulthood study, a 20 year longitudinal cohort that has been followed from adolescence to adulthood and has been assessed during three separate cycles (phases). The original subjects, aged 12 - 16 years [n = 1245 adolescents (89% of the total student population)] were recruited in 1989 when they were enrolled in junior high school at a single school district in Pittsburgh, PA and followed for a period of four years (Phase I). The cohort consisted of similar numbers of male (n = 641) and female (n = 604) adolescents; and the racial composition was 73% white, 24% African American, and 3% Hispanic or Asian [15-17]. In 1999, subjects were re-contacted (aged 22 - 25 years of age) to participate in a follow-up study to examine changes in physical activity from adolescence to young adulthood (Phase II). A total of 827 (66%) completed an interviewer-administered, follow-up questionnaire which included information about health behaviors (i.e., smoking, drug and alcohol use, sedentary behavior), physical activity. Each phase of the current study was approved by the University of Pittsburgh Institutional Review Board and written informed consent was obtained from all participants and/or their parents prior to participation in any part of the study.
2.2. Physical Activity Measures
Physical activity (PA) was assessed using the Modifiable Activity Questionnaire for Adolescents (MAQ-A) [18] and the Modifiable Activity Questionnaire (MAQ). The MAQ-A is an adolescent-specific questionnaire based on the Modifiable Activity Questionnaire (MAQ) for adults. The MAQ-A has been shown to provide reproducible and valid estimates of past year physical activity in adolescents [15,19]. For each of the four years during Phase I, competitive activities as well as leisure time physical activity data were collected by administering the MAQ-A during the spring of each year. Trained research assistants supervised the students as they completed the questionnaire during their regular physical education class. Students were asked to report the frequency and duration of all activities they participated in at least ten times over the past year. The questionnaire inquired about time spent engaged in competitive activities and leisure time PA. The estimated number of hours spent on average for each activity per day was calculated and the average hours per day of all activities was summed to give an estimate of the total physical activity in hours per week averaged over the past year.
During the 1999 follow-up (Phase II), trained interviewers administered a past year Modifiable Activity Questionnaire (MAQ) [20,21]. The MAQ, an interviewer-administered questionnaire for adults, assesses both leisure and occupational activities similar to the MAQ-A completed in the AIC study. The 1999 version asked participants to indicate activities that they had participated in at least ten times over the past year. For each activity, the months of participation was indicated as well as the average days per week and average minutes per day of participation. To assess occupational (non-leisure) activities, participants were also asked to list all jobs held for over one month during the past year and answered questions related to transporttation to and from work, days per week and hours per day of work, time spent sitting, and intensity of non-sitting work related activities.
2.3. Health Risk Behaviors
Health risk behaviors were assessed during years 1, 2, and 4 of Phase I using the Center for Disease Control and Prevention’s Youth Risk Behavior Survey [22] which has been tested for reliability and validity [23]. The health risk behavior questions used in this analysis measured tobacco, alcohol, and binge drinking in the past 30 days. Identical questions were used during the Phase II follow-up phone interview.
2.4. Body Mass Index
During the Phase I, height (cm) and weight (kg) were measured annually with a standard balance scale and used to calculate body mass index (BMI; kg/m2). Shoes were removed prior to all measurements of height and weight. During the Phase II follow-up, BMI was calculated from self-reported height and weight on the questionnaire.
2.5. Statistical Methods
Only participants that had BMI and complete physical activity data at all time-points during Phase I and Phase II (years 1990-1993 and 1999/2000) were included in the analyses. All continuous data were assessed for normality. Normally distributed data are reported as mean (SD), non-normal variables as median (Interquartile range). Categorical data are presented as percentages. Descriptive statistics were calculated for the total cohort and sex-specific grouping. Comparisons between sexes of continuous variables were assessed using a twosample t-test or the Wilcoxon test. Categorical variables were assessed using the Pearson chi-square test. Evaluation of the change in HRB from adolescence to adulthood was performed using a Mc-Nemar’s test.
A series of gender-specific logistic regression models were utilized to evaluate the independent impact of PA, BMI, and adolescent health risk behavior (HRB) on adult HRB. Independent variables included in the regression analyses were treated categorically. Gender-specific physical activity levels were divided into “high” and “low” groups using a median split. BMI was categorized into “normal” (<25.0 kg/m2) and “overweight/obese” (≥25.0 kg/m2) according to NHLBI BMI guidelines [24]. Adolescent health risk behaviors were coded as “never” and “ever” for each heath risk behavior of interest (smoking, drinking, and binge drinking). The outcome of interest, adult HRB, was also coded as “never” and “ever” for each heath risk behavior of interest (smoking, drinking, and binge drinking) during the four year period. Separate univariate models for each HRB of smoking, drinking, and binge drinking were constructed for PA alone, BMI alone, and adolescent health risk behavior alone. The next series of models were conducted using a combination of variables. Model 4 included PA and BMI. Model 5 included PA and adolescent health risk behavior and Model 6 included BMI and adolescent health risk behavior. The final model included PA, BMI, and adolescent HRB. We tested for statistical interactions between physical activity and adolescent health risk behavior by adding a two-way interaction term to the model. Assessment of these interactions was determined by examining the individual p-values of the interaction coefficients and by assessing the impact of the addition of this term to the overall fit of the model. Statistical analyses were performed using Statistical Analysis Software, version 8.2 (SAS Institute Inc., Cary, North Carolina). Statistical significance was considered as a p-value <0.05.
2.6. Study Population
A total of 1245 individuals participated in Phase I, of which 828 participants (67% of original Phase Icohort) completed a follow-up questionnaire, in adulthood, as part of the Phase II. Complete data were available for 536 participants (Figure 1).
Descriptive statistics for the 536 subjects are provided from Phase I (Table 1(a)) and Phase II (Table 1(b)). The mean age of the cohort at the Phase II was 24.8 (±1.1) years with an even split between males and females. Overall, the sample was predominately Caucasian with approximately 74.3% reporting working full time and 62.4% reporting a degree past high school. The average adolescent BMI was 22.5 kg/m2 and increased to 25.4 kg/m2 during adulthood. Physical activity for the total cohort decreased from a median of 12.9 hours per week during adolescence to 5.6 hours per week during young adulthood (Tables 1(a)-(b)).

Figure 1. Flow of subjects.
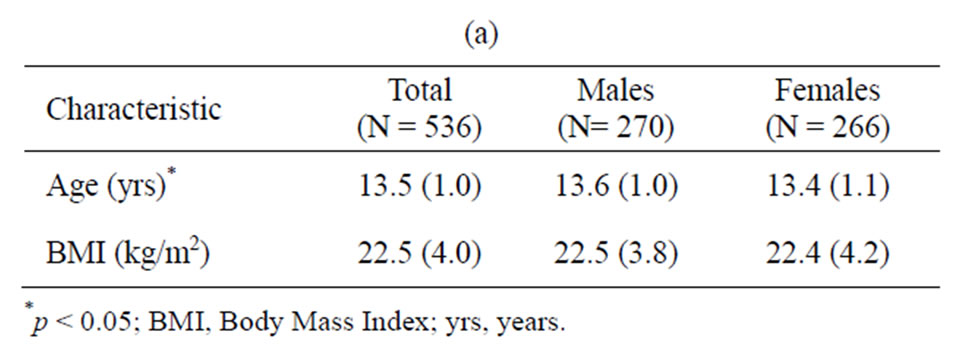
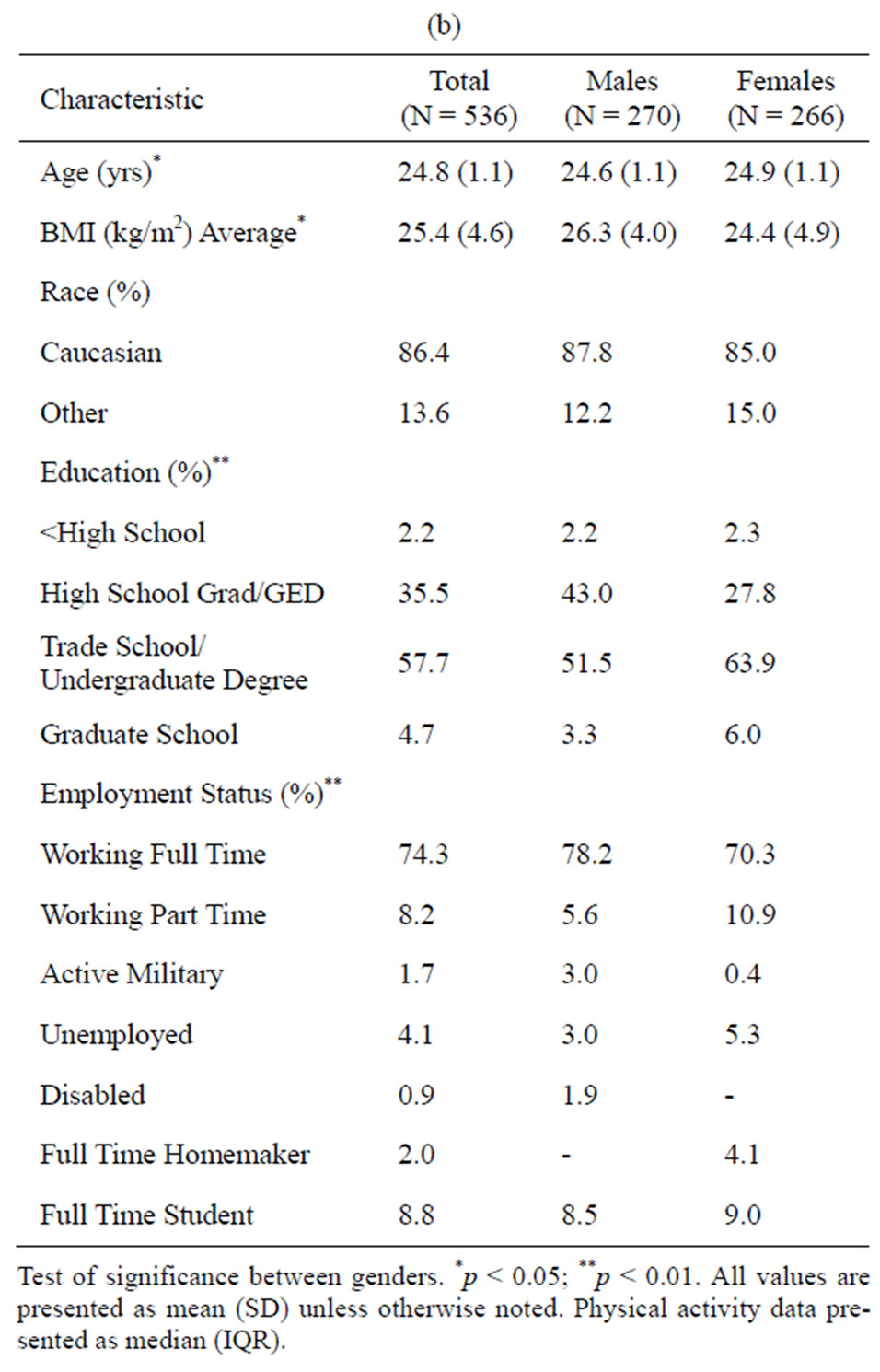
Table 1. Descriptive statistics of the total cohort and stratified by gender for Phase I. Descriptive statistics of the total cohort and stratified by gender for Phase II.
3. RESULTS
Table 2 presents the frequency and percent of subjects engaged in health risk behaviors during adolescence and young adulthood. Approximately 66% of all adolescents reported drinking alcohol during the past 30 days. Drinking during adolescence appears to be similar between boys and girls, however significantly more men than women reported drinking during young adulthood. The prevalence of drinking and binge drinking was significantly higher in adulthood compared to adolescence for both genders. Males reported significantly higher levels of binge drinking at both time periods when compared to females. The

Table 2. Percent reporting health risk behavior during adolescence and young adulthood.
percent of males who smoked during adulthood was significantly higher than that of females with no significant differences noted between genders during adolescence.
Gender-specific logistic regression models for PA, BMI and HRB during adolescence predicting HRB in adulthood are presented in Table 3. Univariate models show that males who engaged in health risk behaviors during adolescence were more likely to continue these same risk behaviors during adulthood (3.68 times more likely to drink, 2.82 times more likely to binge drink and 7.10 times more likely to smoke) than males who did not take part in these risk behaviors during adolescence. In addition, compared to active males, males that were inactive during adolescence were 0.39 times as likely to drink in adulthood (95% CI: 0.18 - 0.83). With regard to females, adolescent smokers and drinkers were more likely (3.38 and 1.75 times, respectively) to continue these behaviors in adulthood compared to those who did not engage in the behaviors during adolescence. When multivariate models were constructed including adolescent PA, BMI and HRB together in the model, only HRB in adolescence predicted HRB in adulthood for drinking, binge drinking and smoking among males, and for binge drinking and smoking among females.
4. CONCLUSIONS
The purpose of the present study was to determine whether higher levels of physical activity and/or having a healthy body weight in adolescence influences the presence of future health risk behaviors such as smoking, drinking and binge drinking during young adulthood. Our results indicate previous engagement in health risk behavior, and not physical activity (PA) level or BMI, is a more important predictor of future health risk behavior in young adulthood. When PA, BMI, and adolescent health risk behaviors are included together in the model, PA and BMI no longer significantly impact drinking, binge drinking or smoking behaviors, respectively.
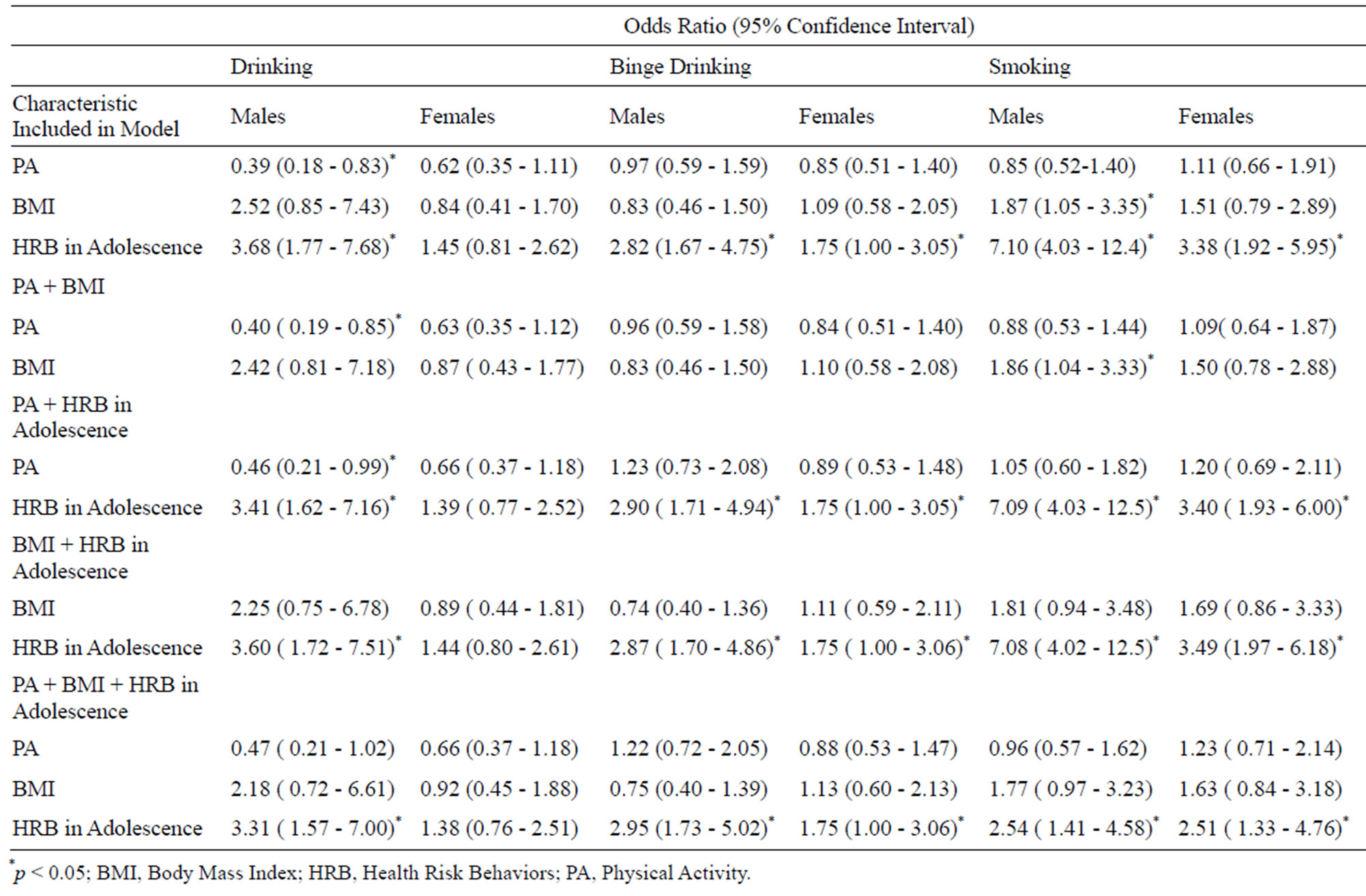
Table 3. Logistic models for predicting health risk behavior in adulthood.
A growing body of intervention literature suggests an association between exercise, often vigorous intensity, with less smoking [13,25-28]. Exercise has been thought to help with smoking cessation because of its association with reduced negative affect, a key component to behavioral interventions [13,29-31]. Other research has found that when exercise is included in the intervention, participants maintained abstinence from smoking longer then non-exercising participants [13] possibly through the reduction of anxiety [32]. However, in this particular cohort, where the natural progression of smoking from adolescence to adulthood is examined, PA appeared to have no influence on smoking behavior. More importantly, if a student engages in smoking during adolescence, they are more likely to continue smoking in adulthood regardless of their PA levels. The differences in the associations seen between the previous studies and ours may be related to the fact that we are examining the natural history of smoking over a protracted period and not as a result of an intervention. Also, it is noted that our study population had higher percentages of risk-taking behaviors during the adolescent years than those reported by YRBSS and BRFSS for the nation [4,5].
The results indicated that HRB during adolescence predicts HRB during young adulthood among males for drinking, binge drinking and smoking, and for binge drinking and smoking among females. These findings were true even after adjustment for PA and BMI during adolescence. Evidence suggests that engagement in risk behaviors during adolescence is correlated with future risk taking behaviors. This is an important finding since other research has indicated that those starting to drink prior to age 15 are four times more likely to meet the criteria for alcohol dependence at some point in their life [33].
In conclusion, it appears that for males, once a healthrisk behavior is initiated, it will likely continue into young adulthood, regardless of the presence of other healthy behaviors such as the proper maintenance of body weight and higher levels of physical activity. Similarly for females, binge drinking and smoking in adolescence is predictive of the same behavior in adulthood. Interventions during adolescence should heavily promote abstinence of these HRB. There appears to be no cross-over benefit of having a healthy weight and increased physical activity levels in regard to smoking and drinking.
REFERENCES
- Mokdad, A.H., Marks, J.S., Stroup, D.F. and Gerberding, J.L. (2004) Actual causes of death in the United States, 2000. JAMA, 291, 1238-1245. doi:10.1001/jama.291.10.1238
- Centers for Disease Control and Prevention (2002) Surveillance summaries, June 28, 2002. MMWR, 51.
- Pape, H. and Hammer, T. (1996) How does young people’s alcohol consumption change during the transition to early adulthood? A longitudinal study of changes at aggregate and individual level. Addiction, 91, 1345- 1357. doi:10.1111/j.1360-0443.1996.tb03620.x
- National Institute on Alcohol Abuse and Alcoholism [NIAAA] (2009) YRBS: Prevalence of binge drinking in the past 30 days, by grade and sex, United States, 1991-2007. http://www.niaaa.nih.gov/Resources/DatabaseResources/QuickFacts/Youth/Pages/ythdrk6b.aspx
- Center for Disease Control [CDC] (2010) National Center for Chronic Disease Prevention and Health Promotion (updated 11/25/2008). Behavior Risk Factor Surveillance System. About the BRFSS. http://www.cdc.gov/brfss/about.htm
- Fan, A.Z., Russell, M., Stranges, S., Dorn, J. and Trevisan, M. (2008) Association of lifetime alcohol drinking trajectories with cardio metabolic risk. The Journal of Clinical Endocrinology & Metabolism, 93, 154-161.
- Oesterle, S., Hill, K.G., Hawkins, J.D., Guo, J., Catalano, R.F. and Abbott, R.D. (2004) Adolescent heavy episodic drinking trajectories and health in young adulthood. Journal of Studies on Alcohol, 65, 204-212.
- Laitinen, J., Pietilainen, K., Wadsworth, M., Sovio, U. and Jarvelin, M.R. (2004) Predictors of abdominal obesity among 31-year old men and women born in Northern Finland in 1966. European Journal of Clinical Nutrition, 58, 180-190. doi:10.1038/sj.ejcn.1601765
- Saarni, S.E., Pietilainen, K., Kantonen, S., Rissanen, A. and Kaprio, J. (2009) Association of smoking in adolescence with abdominal obesity in adulthood: A follow-up study of 5 birth cohorts of Finnish twins. American Journal of Public Health, 99, 348-354. doi:10.2105/AJPH.2007.123851
- Pajari, M., Pietilainen, K.H., Kaprio, J., Rose, R.J. and Saarni, S.E. (2010) The Effect of alcohol consumption on later obesity in early adulthood—A population-based longitudinal study. Alcohol & Alcoholism, 45, 173-179. doi:10.1093/alcalc/agp090
- Wang, L., Lee, I.M., Manson, J.E., Buring, J.E. and Sesso, H.D. (2010) Alcohol consumption, weight gain, and risk of becoming overweight in middle-aged and older women. Archives of Internal Medicine, 170, 453-461. doi:10.1001/archinternmed.2009.527
- Kendzor, D.E., Dubbert, P.M., Oliver, J., Businelle, M.S. and Grothe, K.B. (2008) The influence of physical activity on alcohol consumption among heavy drinkers participating in an alcohol treatment intervention. Addictive Behaviors, 33, 1337-1343. doi:10.1016/j.addbeh.2008.06.013
- Tart, C.D., Leyro, T.M., Richter, A., Zvolensky, M.J., Rosenfield, D. and Smits, J.A. (2010) Negative affect as a mediator of the relationship between vigorous intensity exercise and smoking. Addictive Behaviors, 35, 580-585. doi:10.1016/j.addbeh.2010.01.009
- Marlatt, G.A. (1985) Cognitive factors in the relapse process. In: Marlatt, G.A. and Gordon, J.R., Eds., Relapse Prevention, The Guilford Press, New York, 128-200.
- Aaron, D.J., Storti, K.L., Robertson, R.J., Kriska, A.M. and LaPorte, R.E. (2002) Longitudinal study of the number and choice of leisure time physical activities from mid to late adolescence: Implications for school curricula and community recreation programs. Archives of Pediatrics & Adolescent Medicine, 156, 1075-80.
- Anderson, R., Dearwater, S.R., Olsen, T., Aaron, D.J., Kriska, A.M. and LaPorte, R.E. (1994) The role of socioeconomic status and injury morbidity risk in adolescents. Archives of Pediatrics & Adolescent Medicine, 148, 245- 249. doi:10.1001/archpedi.1994.02170030015003
- LaPorte, R.E., Dearwater, S.R., Chang, Y.F., Songer, T.J., Aaron, D.J., Anderson, R.L. and Olsen, T. (1995) Efficiency and accuracy of disease monitoring systems: Application of capture-recapture methods to injury monitoring. American Journal of Epidemiology, 142, 1069-1077.
- Kriska, A.M. and Caspersen, C.J. (1997) Collection of physical activity questionnaires. Medicine and Science in Sports and Exercise, 29, S79-S82. doi:10.1097/00005768-199706001-00003
- Aaron, D.J., Kriska, A.M., Dearwater, S.R., Cauley, J.A., Metz, K.F. and LaPorte, R.E. (1995) Reproducibility and validity of an epidemiologic questionnaire to assess past year physical activity in adolescents. American Journal of Epidemiology, 142, 191-201.
- Kriska, A.M. and Bennett, P.H. (1992) An epidemiological perspective of the relationship between physical activity and NIDDM: From activity assessment to intervention. Diabetes/Metabolism Reviews, 8, 355-372. doi:10.1002/dmr.5610080404
- Kriska, A.M., Knowler, W.C., LaPorte, R.E., Drash, A.L., Wing, R.R., Blair, S.N., Bennett, P.H. and Kuller, L.H. (1990) Development of questionnaire to examine relationship of physical activity and diabetes in Pima Indians. Diabetes Care, 13, 401-411. doi:10.2337/diacare.13.4.401
- Kolbe, L.J. (1990) An epidemiological surveillance system to monitor the prevalence of youth behaviors that most affect health. Health Education, 21, 44-48.
- Brener, N.D., Kann, L., McManus, T., Kinchen, S.A., Sundberg, E.C. and Ross, J.G. (2002) Reliability of the 1999 youth risk behavior survey questionnaire. Journal of Adolescent Health, 31, 336-342. doi:10.1016/S1054-139X(02)00339-7
- US Department of Health and Human Services [USDHHS] (2010) Body Mass Index Table 1. http://www.nhlbi.nih.gov/guidelines/obesity/bmi_tbl.htm
- Collingwood, T.R., Sunderlin, J., Reynolds, R. and Kohl, H.W. (2000) Physical training as a substance abuse prevention intervention for youth. Journal of Drug Education, 30, 435-451. doi:10.2190/RVUE-9XW7-TYRQ-EJR8
- Marcus, B.H., Albrecht, A.E., King, T.K., Parisi, A.F., Pinto, B.M., Roberts, M., Niaura, R.S. and Abrams, D.B. (1999) The efficacy of exercise as an aid for smoking cessation in women: A randomized controlled trial. Archives of Internal Medicine, 159, 1229-1234. doi:10.1001/archinte.159.11.1229
- Marcus, B., Albrecht, A., Niaura, R., Abrams, D. and Thompson, P. (1991) Usefulness of physical exercise for maintaining smoking cessation in women. American Journal of Cardiology, 68, 406-407. doi:10.1016/0002-9149(91)90843-A
- Martin, J., Kalfas, K. and Patten, C. (1997) Prospective evaluation of three smoking interventions in 205 recovering alcoholics: One-year results of project SCRAP Tobacco. Journal of Consulting and Clinical Psychology, 65, 190-194. doi:10.1037/0022-006X.65.1.190
- Focht, B.C., Knapp, D.J., Gavin, T.P., Raedeke, T.D. and Hickner, R.C. (2007) Affective and self-efficacy responses to acute aerobic exercise in sedentary older and younger adults. Journal of Aging and Physical Activity, 15, 123-138.
- Penedo, F.J. and Dahn, J.R. (2005) Exercise and wellbeing: A review of mental and physical health benefits associated with physical activity. Current Opinion in Psychiatry, 18, 189-193. doi:10.1097/00001504-200503000-00013
- Reed, J. and Ones, D.S. (2006) The effect of acute aerobic exercise on positive activated affect: A meta-analysis. Psychology of Sport and Exercise, 7, 477-514. doi:10.1016/j.psychsport.2005.11.003
- Brown, R.A., Kahler, C.W., Zvolensky, M.J., Lejuez, C.W. and Ramsey, S.E. (2001) Anxiety sensitivity: Relationship to negative affect smoking and smoking cessation in smokers with past major depressive disorder. Addictive Behaviors, 26, 887-899. doi:10.1016/S0306-4603(01)00241-6
- Grant, B.F. and Dawson, D.A. (1998) Age at onset of drug use and its association with DSM-IV drug abuse and dependence: Results from the National Longitudinal Alcohol Epidemiologic Survey. Journal of Substance Abuse, 10, 163-173. doi:10.1016/S0899-3289(99)80131-X