Open Journal of Anesthesiology
Vol.3 No.4(2013), Article ID:33771,7 pages DOI:10.4236/ojanes.2013.34057
Anesthesia Management for Pulmonary Cryoablation*
![]()
1Department of Anesthesiology, Stony Brook University School of Medicine, New York, USA; 2Department of Surgery, Stony Brook University School of Medicine, New York, USA; 3Department of Radiology, Stony Brook University School of Medicine, New York, USA.
Email: #Zvi.Jacob@stonybrookmedicine.edu
Copyright © 2013 Zvi C. Jacob et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received March 8th, 2013; revised April 9th, 2012; accepted May 1st, 2013
Keywords: Anesthesia Care; Percutaneous Cryoablation Treatment; Lung Cancer; Pulmonary Complications; Pneumothorax; Hemoptysis
ABSTRACT
Lung tumors represent a major health impact globally. Pulmonary cryoablation treatment as a palliative measure for patients with non-operable pulmonary lesions has gained popularity over the last decade. With increasing case load and patients medical status becoming more complex, preparation for pulmonary cryoablation requires the implementation of an enhanced perioperative anesthetic plan. Current literature as well as our institutional experience shows that this patient population presents with multiple comorbidities raising the challenge of providing anesthetic care. These procedures are done under challenging conditions with limited resources and in remote locations in the hospital. A team approach by the anesthesiologist, thoracic surgeon, and interventional radiologist is critical to the success of this treatment. The present review examines our institution’s anesthetic management of percutaneous cryoablation treatment (PCT) in the treatment of non-operable lung cancer and metastases. The objective of this article is to review the current literature guidelines and to discuss our retrospective institutional experience in anesthesia management of PCT procedures.
1. Introduction
Primary lung malignancies are the leading cause of cancer mortality. The majority of newly diagnosed patients already suffer from an advanced disease stage. The peak incidence of lung cancer is between the ages 55 and 65. Annually, primary carcinoma of the lungs affects about 93,000 men and 80,000 women in the US with 15% five year survival rate [1].
Percutaneous cryoablation treatment (PCT) is a viable, minimally invasive treatment option for patients with non-small cell lung cancer (NSCLC) or pulmonary metastases [2-4]. Based on our experience, PCT for NSCLC is an excellent palliative alternative for patients who are considered inoperable. An advantage of PCT is that the procedure can be repeated if a patient has a recurrence or a new malignancy. Indications for PCT include patients with lung tumors < 3 cm in size and patients requiring palliation for inoperable lung tumors [4]. PCT has been used with varying degrees of success for treatment of hepatic and renal lesions [5-9]. Interesting applications of this technique have also been described for treatment of endobronchial lesions [2] and neurolysis for chronic post-thoracotomy pain syndromes [10].
PCT has been applied for treatment of pulmonary lesions. Maiwand and Asimakopoulos (2004) [3] reviewed the use of cryotherapy in a group of 15 patients that underwent direct intrathoracic cryosurgery. In their experience there were no post-operative complications resulting from the direct tumor ablation; in fact, dyspnea symptoms improved in 66.7% of patients. In a retrospective report, Zemlyak, Moore & Bilfinger (2010) [4] compared survival after sublobar resection, radiofrequency therapy and percutaneous cryoablation in 64 patients with stage 1 NSCLC. Patients were not randomly assigned to groups; instead, the treatment for each patient was chosen on a case by case basis. Survival after PCT was comparable to outcomes with the other therapies, without serious complications or longterm loss of pulmonary function. In a larger series Wang and colleagues [11] reported 200 procedures performed under local anesthesia with sedation with a 12% incidence of pneumothorax PTX, a 62% incidence of hemoptysis, and a small number of major complications. Unlike other reports, this group used inclusion criteria which did not follow the American College of Surgeons Oncology Group (ACOSOG). This allowed them to include patients with lesions greater than 4 cm in size as well worse pulmonary status, who had previously failed chemotherapy and/or radiation therapy.
Surgical resection is not an option due to poor performance status, comorbidities, and disease status common to patients that qualify for PCT under the American College of Surgery (ACOS) guidelines [4]. Consequently, the anesthesiologist should anticipate significant pulmonary disease and a heightened potential for airway compromise. Better understanding of PCT, the anesthetic management, and potential complications will facilitate a more effective relationship between the anesthesiologist, the thoracic surgeon, and interventional radiologist for improved patient care.
2. Technical Aspects of Cryoablation
Cryoablation, also called cryosurgery, cryotherapy, or percutaneous cryoablation (PCT) is a minimally invasive, localized treatment that uses extreme cold to destroy tumor cells by intracellular and extracellular ice crystal formation. These direct and indirect effects on tumor cells and vasculature result in membrane rupture and cell dehydration [12]. The concept of using cold for tissue destruction of malignant tumors is not novel, as it was attempted in the 19th century [12]. PCT utility has recently increased for a wide range of applications, including the treatment of renal masses, prostate carcinoma, hepatic malignancy, lung cancer, and nerve ablation for pain syndromes, amongst other indications [6-10].
For non-operable lung cancer or metastases, PCT involves inserting a cryoprobe into the lesion of the lung with the goal of local tissue destruction. PCT is most effective for patients with tumors < 3 cm because this is the approximate diameter of cryoablation probes. In our center, cryoablation is performed under CT guidance by an interventional radiologist and thoracic surgeon. An anesthesiologist is present and the patient remains under general anesthesia for the duration of the procedure.
The PCT procedural protocol includes placing a Percryo 17 or Percryo 24 (1.7 mm or 2.4 mm diameter) cryoablation probe (Endocare Cryocare CS, Irvine, CA, USA) into the targeted lesion under CT guidance (see Figure 1). When the probe is in the optimal position as confirmed by CT imaging the ablation is performed (see Figure 2). The standard protocol used for all procedures is a ten minute active freeze cycle with typical temperatures of −160 degrees Celsius, an eight minute “stick” cycle which is an inactive freeze cycle with typical temperatures of −10 degrees Celsius to be followed by a final ten minute active freeze cycle.
The cryoprobe uses high-pressure argon and helium gas for freezing and thawing, respectively, on the basis of the Joule-Thomson principle. During the active freeze cycle argon enters the distal aspect of the probe and passes through a valve. This results in rapid change in the temperature. Close to the probe there is intracellular ice formation. During the 10 minute freeze cycle re-crystallization occurs, which causes super-cooling of the intra-cellular cytoplasm and results in cell death by destruction of the intra-cellular structures. Several millimeters away from the tip of the probe there is a more gradual cooling of the tissues which results in extracellular ice formation. This results in an osmotic gradation and intra-cellular dehydration. During the active warming cycle, when helium is introduced to the tip of the probe there is heating of the probe to +40 degrees C. This results in shifts of fluid into the cell and cellular lysis.
At the cellular level, the fast freezing cycle creates ice crystals inside and outside the cells. During the fast thawing phase, helium gas is introduced and cracks the lethal ice. As a result, the cell mitochondria disappear, and the membranes are split causing cell death. PCT also causes transcellular electrolytes and osmotic pressure imbalance furthering local cell destruction.

Figure 1. Percutaneous cryoprobe creating an ice ball. Probe manufactured by Endocare Cryocare CS, Irvine, CA, USA.
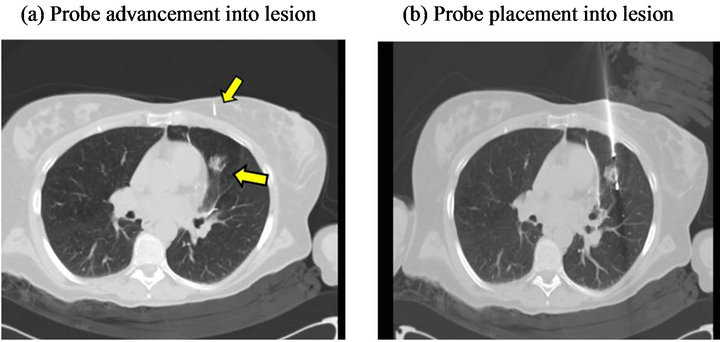
Figure 2. Image of thoracic cavity with cryoprobes inserted under CT guidance. (a) Lung lesion; (b) Cryoprobe inserted into lesion.
Air in the lung can interfere with the creation of the ice ball. Positioning of the probe into the lesion is critical for the freezing process as the air in the lung will act as an insulator, thus limiting the extent of the freeze. Cellular reperfusion injury, which takes place during the thawing phase may also account for more tumor tissue destruction and necrosis [12].
3. Anesthesia Management
The anesthetic management of a patient presenting for PCT is similar to the common guidelines and principles applied for patients undergoing a surgical procedure. Understanding of the patient’s basic pathology, comorbidities, their expected impact on the anesthesia care, and the procedure itself is essential for patient safety. All patients at our institution visit Pre-Anesthesia Testing prior to the procedure. A comprehensive medical history and physical assessments are obtained, with specific attention to coexisting illness and cardiopulmonary reserve. Required laboratory evaluations include: electrocardiogram, chest X-ray, and laboratory tests, including complete blood cell count and chemistry profile. If additional information is needed, it is ordered at this time. At this visit, the patient is counseled regarding the anesthesia risk, fasting guidelines, and anticipated anesthetic technique.
In our institution, almost all of our patients are admitted on the same day of the procedure. After placement of a peripheral intravenous line, premedication in the form of intravenous midazolam is typically given. Attention should be directed towards the patient’s pulmonary status and the potential risk for airway obstruction and hypoventilation. The patient is brought to the interventional radiology suite and positioned on a stretcher. Monitoring includes standard ASA monitors: ECG, pulse oximeter, noninvasive automated blood pressure cuff, temperature probe and capnography.
General anesthesia induction with endotracheal intubation is performed prior to the final positioning on the CT imaging bed. The method of securing an airway in this patient population requires multiple considerations. In special circumstances such as when difficult intubation or lung separation is indicated, it is essential to coordinate availability of advanced airway equipment and support as most of these procedures are taking place at a remote location in the hospital. At the discretion of the anesthesiologist additional access lines and monitors may include extra-large bore intravenous access, invasive arterial blood pressure monitoring, and central venous pressure monitoring.
Patient positioning is an important part of PCT cases. Depending on the target area of the lesion, patients may be positioned prone, supine, or laterally. Attention should be directed towards the fall risk as the radiology suite’s procedure beds are generally narrower than the standard operative beds increasing the risk for fall injuries. It is important to protect the patient’s body, specifically the upper extremities, from potential injury caused by the scanner bore while the bed is moving the patient in and out of position. Greater emphasis on this particular consideration should be given for obese patients with a BMI greater than 40. Appropriate padding and support should be available for positioning patients in the prone or lateral position (see Figure 3).
Anesthesia maintenance can be achieved using a balanced technique combining volatile agents, muscle relaxants, and narcotic analgesics. Volatile agents such as sevoflurane or desflurane have a relatively fast onset and offset, function as bronchodilators, and allow for better hemodynamic control appropriate for this type of procedure. Short or intermediate-acting muscle relaxants (e.g. rocuronium, vecuronium) are appropriate to facilitate patient positioning and mechanical ventilation. Narcotics should be carefully administered maintaining a balance between appropriate analgesia management and the risk for post-procedure hypoventilation.
Due to the minimally invasive nature of this procedure, the expected heat loss is minor. Some heat loss is expected due to vasodilation caused by anesthetics and exposure to cool room air. The risk of hypothermia is minimized by the short duration of anesthesia for the PCT procedure. Furthermore, there is no documentation regarding major heat loss from the cryoprobe during the procedure. Active warming devices, such as convective heating blankets, warm IV fluids, or circuit moisture devices, are not used routinely but may be considered for cases longer in duration. Use of a convective heating system presents a potential concern while moving the bed into the scanner bore.

Figure 3. Patient positioned prone for PCT.
4. Post-Procedure Phase
Immediate post-operative complications are strongly related to intraoperative airway thermo-trauma and bleeding. After meeting standard extubation criteria, ETT and lower airway suctioning followed by early extubation in the procedure room is strongly recommended. More extensive procedures may result in a more complicated clinical course in the immediate post-procedure period, such as PTX, severe hemoptysis, and severe airway irritation. These complications may require temporary ventilatory support (typically < 6 hours) and insertion of a chest tube. All patients typically recover in the main post anesthesia care unit (PACU). Regardless of the intraoperative course, these patients should be provided with intensive postoperative follow up due to the inconsistent nature of post-procedural complications associated with PCT. Acute post-procedural pain is expected from the probe insertion site and chest tube placement. Almost all patients will require pain management in the form of narcotics. The anesthesiologist should be aware of the high risk for post-procedure hypoventilation associated with narcotic use. Most patients will require 24 hours admission post-procedurally for pain management and monitoring for PTX.
5. Our Experience
Our retrospective review included 53 patients with lung cancer who underwent 69 PCT treatments under anesthesia at Stony Brook University Hospital between January 2006 and January 2011. These patients are substantially the same cohort previously reported on by Zemlyak, Moore & Bilfinger (2010) [4]. All these patients met at least one major or two minor criteria of the American College of Surgeons Oncology Group (ACOSOG) for inoperability (www.acosog.org) and had been reviewed by a tumor board. After obtaining IRB approval, we extracted information from the electronic medical records and reviewed anesthesia records. The following data were recorded: gender, age, ASA status, co-morbidities, medications, diagnosis, treatment area, positioning, use of invasive monitoring, airway management, complications, fluid management, anesthetic technique, and length of stay.
The patients’ mean age at time of treatment was 69 years, 58% of patients were female, 75.4% of patients were ASA III and the remainder were ASA IV. The majority of the patients were diagnosed with non-small cell lung cancer, with 24.6% of patients having metastases at the time of treatment (Table 1).
Table 2 gives the information on the anesthetic management of our cases. Advanced airway techniques were utilized in 10% of cases. These techniques included a Bougie guide, fiberoptic guided intubation, and retrograde bronchoscopy; a double lumen endotracheal tube was used in two cases. In our population patients were positioned for the procedure most often in the lateral position, followed by the supine and prone positions. Cen-

Table 1. Patient characteristics.

Table 2. Anesthetic management.
tral venous lines for medication access and arterial lines for monitoring were placed in 2.9 and 26.1 percent of patients, respectively. All procedures were performed under general anesthesia and patients were required to stay overnight after treatment to allow early detection and mitigation of complications.
The choice of anesthetic technique was at the discretion of the attending anesthesiologist. In nearly all cases (94%) anesthesia was maintained using a balanced technique with inhalational volatile agents, muscle relaxants, and narcotic analgesics. For induction, propofol or etomidate was used followed by a neuromuscular blocking agent (succinylcholine, rocuronium or vecuronium). Midazolam was used as a premedication and fentanyl was used to blunt response to laryngoscopy in the majority of cases. The volatile anesthetics used were sevoflurane (63.3%) and desflurane (36.7%). The choice of anesthetic technique was not associated with the procedure’s outcome or rate of complications. The majority of the procedures (53.2%) were 2 - 3 hours in length, followed by 1 - 2 hours (41.9%), and three cases (4.8%) needed more than 3 hours to be completed.
Complications, although frequent, were relatively minor. Delayed extubation was indicated in thirteen procedures (19%), and the patients were extubated in PACU. These patients were more likely to suffer from pulmonary comorbidities (10 of 13 cases, p = 0.047 by chisquare). Twenty six patients (37.7%) had a pneumotho- rax and were treated conservatively; three patients (4.3%) were treated by chest tube insertion (Table 3).
Pneumothorax was unrelated to BMI (see Figure 4) but occurred more frequently in patients treated in the lateral position. As shown in Figure 5, PTX was seen in 4 of 19 patients (21.1%) in the prone position and 5 of 11 patients in the supine position (31.3%), but occurred in 16 of 27 patients (59.3%) in the lateral position (P = 0.023 by chi-square). PTX developed twice as often for right-sided lesions (10 of 16 cases) treated in the lateral position as for left sided lesions (5 of 16 cases). Cases of PTX were unrelated to which lung side was the dependent side.
Seventeen patients (24.6%) had hemoptysis (Table 3) which was treated by airway suctioning, and in two cases, hemorrhage was significant enough to halt the procedure.

Table 3. Complications after cryoablation.
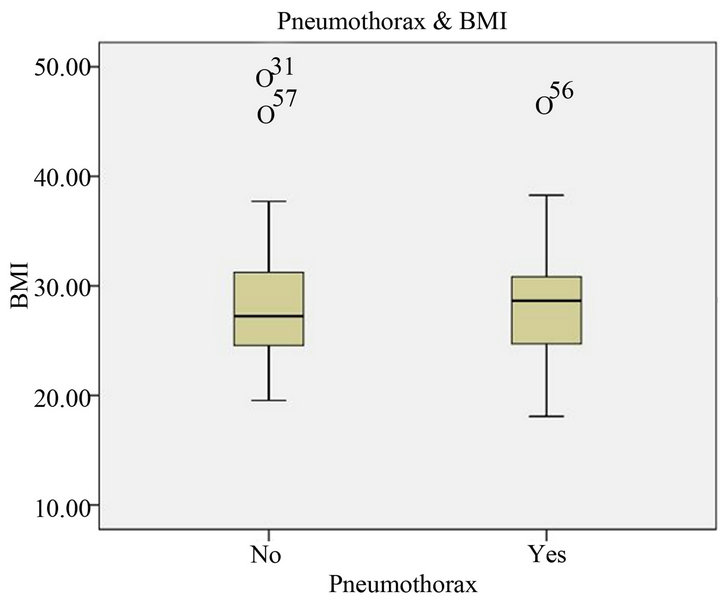
Figure 4. Body mass index (BMI) values in patients with and without pneumothorax (PTX). This plot indicates the distribution of data values (solid line in box is the mean). Outliers (beyond 3 interquartile ranges) are indicated by circles and identified by subject ID number. The figure shows clearly that patients with and without PTX did not differ in BMI.

Figure 5. Incidence of pneumothorax (PTX) by surgical positioning. PTX is more frequent in patients treated in the lateral position (P = 0.023 by chi-square test).
(see Figure 6). Five patients were classified as suffering “severe complications” which included significant bleeding with pneumothorax. One patient suffered major intrapulmonary hemorrhage with a large pneumothorax. After placement of a chest tube and initial hemodynamic support, the patient was admitted to the MICU intubated and sedated. The patient expired 48 hours later due to sudden cardiac arrhythmia deemed unrelated to the procedure. Regardless, the majority (71%) of patients were discharged from the hospital within 24 hours post-procedure. 19% were discharged on day 3 and the remainder required longer hospital stays.
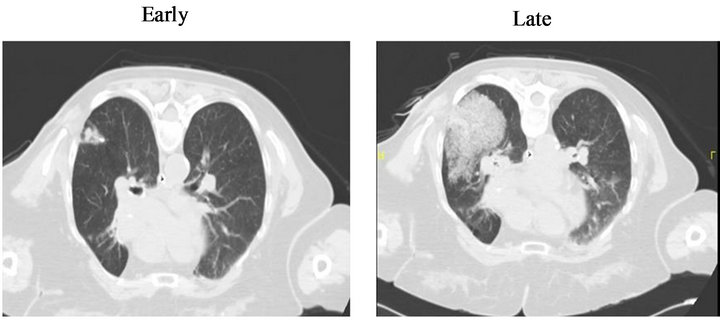
Figure 6. Development of post-procedural alveolar hemorrhage. (a) Early; (b) Late.
6. Summary and Conclusions
Percutaneous cryoablation treatment (PCT) is a minimally invasive technique to treat non-operable lung malignancies and metastases. PCT can be done under local or general anesthesia, or moderate sedation. The anesthesiologist must be cognizant of the patient’s comorbidities and understand the procedure well enough to anticipate potential complications. This review serves as an introduction to the role of the anesthesiologist in PCT by outlining the experience from our center.
In our center, 53 ASA III and IV patients underwent 69 cryoablation procedures. Our management required the presence of an attending anesthesiologist throughout the procedure. All patients received balanced general anesthesia with endotracheal intubation. Advanced airway modalities were utilized in 10.1% of procedures. Delayed extubation occurred in 13% of cases. The complications of the procedure while frequent were relatively minor to moderate severity; 37.7% of patients had a pneumothorax, 24.6% had hemoptysis, and 4.3% of patients needed chest tube insertion. There was one mortality from cardiac arrhythmia which occurred in the MICU 48 hours after the procedure and was deemed unrelated to the PCT.
In our center we chose to perform PCT under general anesthesia in order to create the best and safest conditions for probe placement. Other teams report using local anesthesia combined with mild sedation. Kawamura and colleagues [13] performed 22 PCTs on 20 patients all under local anesthesia with minimal sedation using atropine sulfate (0.5 mg IM) and pentazocine (15 mg IM). They reported PTX in 11 procedures (50%) requiring chest tube placement for 1 patient (4.5%), and hemoptysis in 8 patients (36%). The mean hospital stay was 2.6 days (range, 2 - 6 days). Wang and colleagues [11] reported 200 procedures performed under local anesthesia with lidocaine; most patients received no sedation. When used, sedation was provided with morphine 2 - 4 mg with or without midazolam. This group reported a 12% incidence of PTX, a 62% incidence of hemoptysis, and a small number of major complications. In our case series, we observed 37.7% PTX and 24.6% hemoptysis. We recommend that GA be used to increase the safety margin. General anesthesia is preferable to other techniques when procedures are performed on medically challenging patients at a remote location in the hospital with limited resources and assistance for emergency intervention.
One of the main concerns from an anesthesia perspective is that patients with severe emphysema or other pulmonary comorbidities may show significant intraalveolar hemorrhage and/or pneumothoraxes requiring a delayed extubation. Vricella and co-workers noted that the complication rate in their patient cohort was predicted by Charlson Comorbidity score, and suggest that ASA classification may be used as a substitute where Charlson Comorbidity score is not available [9]. However, we found no relationship of ASA status or prior comorbidities with complications of PTX, hemoptysis or chest tube placement. Other studies have indicated similar and even higher rates of pneumothorax and hemoptysis. Bleeding may be anticipated to occur with thawing, especially if the ice ball should crack. Some authors argue that hemoptysis may be inevitable after cryotherapy because it may indicate a death of endothelial cells and rupture of capillaries [12].
Interestingly, our case series showed a relationship between PTX and lateral positioning for the procedure. We have no specific explanation for this incidental finding. However, pulmonary lesions approached through a lateral approach tend to be closer to the surface than lesions approached from an anterior-posterior direction. The thoracic cage and the lungs move more in a lateral position than in an anterior-posterior position. Further, it may have to do with a more difficult anatomical approach for lesions which are near vital structures. We have reviewed the clinical literature on cryoablation for pulmonary tumors and find that the important case series to date have not addressed the issue of patient positioning for treatment [2-4,11,13]. For ablation of renal or hepatic lesions, patients are placed in the prone position and pulmonary complications are generally absent. Since our data indicate that PTX is not associated exclusively with the lateral position, but approximately one of three cases occur in the prone or supine position, it is not surprising that this association has escaped the notice of clinicians. Further research is needed to clarify whether there is a causal relationship between the lateral position and occurrence of PTX.
Complications may also be related to the position of the tumor. Only relatively superficial lesions are candidates for percutaneous cryoablation, and we select patients with tumor size < 3 cm. We found no association between side (R vs L) or lobe (upper, middle, lower) of lung and occurrence of PTX or hemoptysis. However, Vricella et al. (2010) [9] noted that postoperative hemorrhage was related to the number of probes placed for cryoablation. In our data we also observed a trend for more severe complications (moderate or severe pneumothorax or hemorrhage) to be associated with placement of multiple cryoprobes (P = 0.080 by Fisher’s exact test, one-tailed). Patients who returned for multiple treatments were no more likely to experience severe complications than patients who underwent only one treatment.
In our experience, PCT should be performed under general anesthesia with a team approach from the anesthesiologist, thoracic surgeon, and interventional radiologist. PCT may be performed under local anesthesia, moderate sedation or general anesthesia; however, we prefer to provide general anesthesia. Since the patients undergoing this procedure are typically older with several comorbidities, the anesthesiologist should understand the intricacies of PCT in order to safely respond to potential complications. Additional research and attention needs to be placed on PCT because anesthesiologists can expect increasing involvement in minimally invasive procedures on patients with many comorbidities.
7. Acknowledgements
We acknowledge Christopher Biel B.S. for his assistance in this project.
REFERENCES
- J. D. Minna, “Neoplasms of the Lung,” In: D. L. Dennis, E. Braunwald, A. S. Fauci, S. L. Hauser, D. L. Longo and J. L. Jameson, Eds., Harrison’s Principles of Internal Medicine, McGraw-Hill Professional, Blacklick, 2005, pp. 506-515.
- G. Asimakopoulos, J. Beeson, J. Evans and M. O. Maiwand, “Cryosurgery for Malignant Endobronchial Tumors,” Chest, Vol. 127, No. 6, 2005, pp. 2007-2014. doi:10.1378/chest.127.6.2007
- M. O. Maiwand and G. Asimakopoulos, “Cryosurgery for Lung Cancer: Clinical Results and Technical Aspects,” Technology in Cancer Research and Treatment, Vol. 3, No. 2, 2004, pp. 143-150.
- A. Zemlyak, W. H. Moore and T. V. Bilfinger, “Comparison of Survival after Sublobar Resections and Ablative Therapies for Stage I Non-Small Cell Lung Cancer,” Journal of the American College of Surgeons, Vol. 211, No. 1, 2010, pp. 68-72. doi:10.1016/j.jamcollsurg.2010.03.020
- D. B. Goodie, M. D. Horton, R. W. Morris, L. S. Nagy and D. L. Morris, “Anaesthetic Experience with Cryotherapy for Treatment of Hepatic Malignancy,” Anaesthesia and Intensive Care, Vol. 20, No. 4, 1992, pp. 491-496.
- K. Littlewood, “Anesthetic Considerations for Hepatic Cryotherapy,” Seminars in Surgical Oncology, Vol. 14, No. 2, 1998, pp. 116-121. doi:10.1002/(SICI)1098-2388(199803)14:2<116::AID-SSU4>3.0.CO;2-8
- K. Miki, T. Shimomura, H. Yamada, K. Kishimoto, Y. Ohishi, J. Harada and S. Egawa, “Percutaneous Cryoablation of Renal Cell Carcinoma Guided by Horizontal Open Magnetic Resonance Imaging,” International Journal of Urology, Vol. 13, No. 7, 2006, pp. 880-884. |doi:10.1111/j.1442-2042.2006.01432.x
- T. S. Ravikumar and G. D. Steele Jr., “Hepatic Cryosurgery,” Surgical Clinics of North America, Vol. 69, 1989, pp. 433-438.
- G. J. Vricella, J. R. Haaga, B. L. Adler, D. Nakamoto, E. E. Cherullo, S. Flick and L. E. Ponsky, “Percutaneous Cryoablation of Renal Masses: Impact of Patient Selection and Treatment Parameters on Outcomes,” Urology, Vol. 77, No. 3, 2010, pp. 649-654. doi:10.1016/j.urology.2010.08.016
- M. Moore, D. Kolnick, J. Tan and H. S. Yu, “CT Guided Percutaneous Cryoneurolysis for Post Thoracotomy Pain Syndrome,” Academic Radiology, Vol. 17, No. 5, 2010, pp. 603-606. doi:10.1016/j.acra.2010.01.009
- H. Wang, P. J. Littrup, Y. Duan, Y. Zhang, H. Feng and Z. Nie, “Thoracic Mass Treated with Percutaneous Cryotherapy: Initial Experience with More than 200 Procedures,” Radiology, Vol. 235, No. 1, 2005, pp. 289-298. doi:10.1148/radiol.2351030747
- N. E. Hoffman and J. C. Bischof, “The Cryobiology of Cryosurgical Injury,” Urology, Vol. 60, No. 2a, 2005, pp. 40-49. doi:10.1016/S0090-4295(02)01683-7
- M. Kawamura, Y. Izumi, N. Tsukada, K. Asakura, H. Sugiura, H. Yashiro, K. Nakano, S. Nakatsuka, S. Kuribayashi and K. Kobayashi, “Percutaneous Cryoablation of Small Pulmonary Malignant Tumors under Computed Tomographic Guidance with Local Anesthesia for Nonsurgical Candidates,” Journal of Thoracic and Cardiovascular Surgery, Vol. 131, No. 5, 2006, pp. 1007-1013. doi:10.1016/j.jtcvs.2005.12.051
NOTES
*The authors received no financial support from grants or other funding sources.
#Corresponding author.