Open Journal of Urology
Vol.06 No.10(2016), Article ID:71611,5 pages
10.4236/oju.2016.610026
A Pelvic Free-Floating “Intraperitoneal Mice” Mimicking Seminal Vesicle Malignancy: A Case Report
Abdelghani Ammani1,2*, Abdelmonaim Qarro1,2, Jamal Laaroussi3, Mohammed Lezrek2, Mohammed Alami1,2
1Department of Urology, Medical School, University Sidi Mohammed Benabdellah, Fez, Morocco
2Department of Urology, Moulay Ismail Military Hôspital, Meknes, Morocco
3Department of Surgery, Moulay Ismail Military Hospital, Meknes, Morocco

Copyright © 2016 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY 4.0).
http://creativecommons.org/licenses/by/4.0/



Received: May 20, 2016; Accepted: October 25, 2016; Published: October 28, 2016
ABSTRACT
Peritoneal loose bodies or “peritoneal mice” are rare well circumscribed benign masses composed of free-floating organized fat necrosis. They are usually asympto- matic and found as “incidentalomas” during Imaging. Their pathogenesis is not well known. We report a rare case of giant intraperitoneal mice which was clinically misdiagnosed as left seminal vesicle malignancy. A review of the literature is also presented.
Keywords:
Peritoneal Loose Body, Pathophysiology, Pelvic Mass, Seminal Vesicle, Malignancy, Laparoscopy

1. Introduction
Peritoneal loose bodies or “peritoneal mice” are rare well circumscribed benign masses composed of free-floating organized fat necrosis. They are usually asymptomatic and found as “incidentalomas” during Imaging, laparotomy or autopsy [1] [2] . The path- ogenesis of peritoneal mices is not well known. They are thought to evolve from torsion and separation of the appendices epiploicae. Others have suggested that large loose bodies can be formed by the accumulation of peritoneal serum in the appendices epiploicae [3] [4] .
We report a rare case of giant intraperitoneal mice which was clinically misdiagnosed as right seminal vesicle malignancy and was succesfully managed laparoscopically.
2. Case Presentation
We report the case of a 64-year-old man with no remarkable medical history who presented with six months recurrent hematuria, chronic pelvic pain syndrome (CPPS) and inconstant symptoms of tenesmus. Routine blood tests, including PSA, testosterone and prolactin levels, were normal. Transrectal ultrasonography (TRUS) showed a hyperechoic localized tumor in contact of the right seminal vesicle and a posterior enhancement of central calcification (Figure 1). Computerized tomography scan (CT) and magnetic resonance imaging (MRI) demonstrated an oval well circumscribed retrovesical soft tissue lesion measuring 3.9 × 3.7 × 4 cms with a central negative density (−40.92 UH) and positive peripheral density (+48.17 UH) without enhancement after injection of contrast product. This well-circumscribed egg-shaped lesion seems to be in contact with the right seminal vesicle (Figure 2 and Figure 3).
A diagnostic laparoscopy was performed and revealed an intraperitoneal mobile cream-coloured egg situated between the anterior wall of the rectum and the bladder which was removed via a 4 cm infraumbilical incision (Figure 4).
Histologically, the wall showed concentric lamellar fibrosis and calcification, whereas the nucleus displayed fat necrosis; all consistent with diagnosis of peritoneal loose body. The patient had a favourable recovery and was discharged home the following day. All symptoms of bowel and bladder irritation were relieved postoperatively.
3. Discussion
The pathophysiologic process for the developpement of intraperitoneal free-floatting bodies has not yet been fully elucidated. However, it is generally agreed that peritoneal loose bodies arise from torsion and separation of appendices epiploicae from the antimesenteric taenia of the colon [1] - [3] . First, appendices epiploicae are subjected to torsion and subsequent infarction with inflammatory changes related to peritoneal

Figure 1. Transrectal ultrasonography showing a hyperechoic right laterorectal mass with posterior enhancement of central calcification.

Figure 2. CT scan: oval well circumscribed retrovesical soft tissue lesion with a central negative density (−40.92 UH) and positive peripheral density (+48.17 UH) without enhancement.
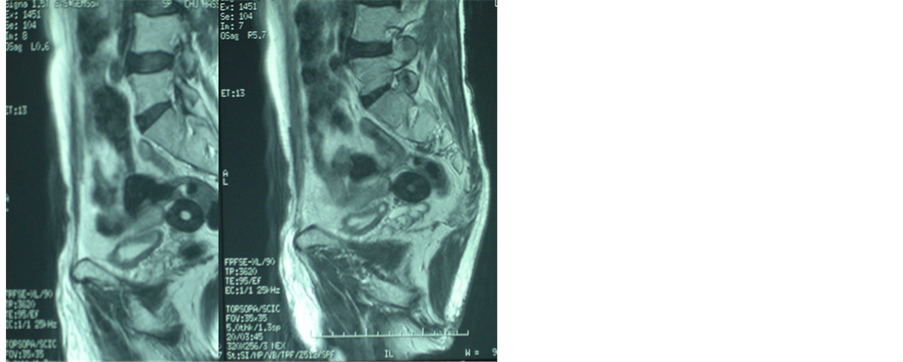
Figure 3. MRI: sagittal image of the pelvis revealing a well- circumscribed egg-shaped lésion measuring 3.9 × 3.7 × 4 cms cm with central calcifications.
adhesions (local peritonitis). Clinically patients presented with an acute abdomen. Diagnosis is often an intraoperative discovery due to inaccuracy of conventional Imaging to eliminate an acute appendicitis, volvulus, occlusion or even intestinal perforation. Secondarily, chronic ischemia by torsion leads to saponification and calcification of fat tissue. Vascular pedicle atrophy results in the detachment of the appendix epiploica which becomes a peritoneal loose body or “peritoneal mice”.
The prevalence of peritoneal loose bodies is not clearly documented and it is not uncommon to find small loose bodies during laparotomy. “Peritoneal mice” is usually

Figure 4. Laparoscopic view of a cream-coloured egg situated between the rectum and the posterior wall of the bladder.
asymptomatic and found as “incidentalomas” during Imaging, laparotomy or autopsy [5] [6] . However, giant loose bodies (>5 cms) are very rare and may causes significant pelvic symptomatology related to mass effect as in our patient [2] [3] [7] . Peritoneal loose body is a histopathologic diagnosis because conventional cross-sectional imaging cannot accurately establish the diagnosis and outrule pelvic neoplasms such as leiomyomas, fibromata, desmoid tumors, teratomas, metastatic lesions of ovarian cancer, calcification of lymph nodes, mesenteric cysts, and rectal or seminal vesicle ma- lignancy [3] [6] . TRUS guided biopsy is difficult and often inconclusive due to cranial migration of the loose bodies which remained not amenable to ultrasonographic visualisation [3] [6] [7] . Laparoscopic retrieval is recommended to alleviate symptoms and outrule malignancy [3] [5] . In our case, laparoscopy was usefull to eliminate a pelvic malignancy, to extracte the loose body and to confirm the diagnosis histologically. After a 3 years follow up, there was no reccurence.
4. Conclusions
Giant peritoneal loose bodies are rare clinical entities. Their physiological significance is unclear and it is generally agreed that it arises from appendices epiploicae. Imaging is often inconclusive and laparoscopic abdomenal exploration is recommended for the management of these incidentalomas.
*Informed consent was obtained from the patient to report this case.
Cite this paper
Ammani, A., Qarro, A., Laaroussi, J., Lezrek, M. and Alami, M. (2016) A Pelvic Free-Floating “Intraperitoneal Mice” Mimicking Seminal Vesicle Malignancy: A Case Report. Open Journal of Urology, 6, 159-163. http://dx.doi.org/10.4236/oju.2016.610026
References
- 1. Koga, K., Hiroi, H., Osuga, Y., Nagai, M., Yano, T. and Taketani, Y. (2010) Autoamputated Adnexa Presents as a Peritoneal Loose Body. Fertility and Sterility, 93, 967-968.
http://dx.doi.org/10.1016/j.fertnstert.2009.03.038 - 2. Rubenstein, J.N., Hairston, J.C., Eggener, S.E. and Gonzalez, C.M. (2002) Irritative Voiding Symptoms and Microscopic Hematuria Caused by Intraperitoneal Calcified Fat Necrosis. Urology, 59, 444.
http://dx.doi.org/10.1016/S0090-4295(01)01599-0 - 3. Kavanagh, D.O., Moran, D., Flynn, R. and Neary, P.C. (2010) Laparoscopic Retrieval of a Peritoneal Mouse. Case Reports in Medicine, 2010, Article ID: 624825.
http://dx.doi.org/10.1155/2010/624825 - 4. Mohri, T., Kato, T. and Suzuki, H. (2007) A Giant Peritoneal Loose Body: Report of a Case. American Surgeon, 73, 895-896.
- 5. Asabe, K., Maekawa, T., Yamashita, Y. and Shirakusa, T. (2005) Endoscopic Extraction of a Peritoneal Loose Body: A Case Report of an Infant. Pediatric Surgery International, 21, 388-389.
http://dx.doi.org/10.1007/s00383-004-1341-1 - 6. Nomura, H., Hata, F., Yasoshima, T., et al. (2003) Giant Peritoneal Loosebody in the Pelvic Cavity: Report of a Case. Surgery Today, 33, 791-793.
http://dx.doi.org/10.1007/s00595-003-2573-8 - 7. Ohgitani, D., Kani, H., Matsuki, M., Kanazawa, S. and Narabayashi, I. (2004) A Case of Giant Peritoneal Loose Body: Usefulness of Wide Window Width CT. Nippon Acta Radiologica, 64, 223-224.