Case Reports in Clinical Medicine
Vol.3 No.3(2014), Article ID:43495,5 pages DOI:10.4236/crcm.2014.33026
Angiosarcoma Thyroid: Case Report and Review of Literature
Aayush Mittal1*, Sunil Kumar2, Yumlembem Brojendro Singh2, Sunil Garg2
1Department of Otorhinolaryngology—Head & Neck Surgery, Hind Institute of Medical Sciences and Shekhar Hospital, Lucknow, India
2Department of Otorhinolaryngology—Head & Neck Surgery, Lady Hardinge Medical College, New Delhi, India
Email: *aayush_mittal@yahoo.com, suku321@rediffmail.com, bzone_amc@yahoo.com, dr.sunilgarg07@gmail.com
Copyright © 2014 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/


Received 5 December 2013; revised 3 January 2014; accepted 2 February 2014
ABSTRACT
Objective: To describe a rare case of angiosarcoma thyroid in Indian subcontinent with its successful management. Case report: A 60-year-old male with swelling in neck for 20years with sudden increase in the size during last 3 months. Fine needle aspiration cytology suggested anaplastic carcinoma. The patient underwent total thyroidectomy with central and lateral neck dissection. On histopathology, the diagnosis of angiosarcoma was suspected. Immunohisto chemistry confirmed the diagnosis of angiosarcoma. Post-operative chemoradiation was given with no recurrence at 10 months of follow up. Conclusion: Though rare, angiosarcoma should be included as differential diagnosis in cases of long standing goiters with recent rapid increase in size. Immunohistochemistry is crucial for diagnosis and should be considered in these patients. Early and prompt diagnosis will help in providing curative treatment in such patients.
Keywords:Angiosarcoma; Thyroid

1. Introduction
Sarcomas are the malignant tumors of mesenchymal origin. As most of the thyroid gland tumors are epithelial in origin, sarcomas are rarely found in thyroid. The various types of sarcomas found in thyroid gland are liposarcoma, angiosarcoma, leiomyosarcoma, dendritic cell sarcoma [1] . Various vascular malignant tumors of the thyroid include angiosarcomas or undifferentiated angiosarcomatoid carcinomas [2] .
Angiosarcoma is one of the rarest soft tissue neoplasm (2%), found mostly in skin and superficial soft tissues [3] . It is rarely seen in thyroid gland. But, it represents 2% - 10% of all thyroid malignancies in European Alpine regions [4] .
Angiosarcoma has anunfavorable prognosis because of rapid local spread and early metastasis. It rapidly involves the regional lymph nodes and sometimes lungs; also rarely the bone marrow [5] . The main line of treatment is radical surgery followed by radiotherapy and sometimes chemotherapy may also be needed [6] .
The diagnosis of this disease entity poses a challenge to clinician due to its rarity. Difficulties are also encountered by the pathologist due to its histopathological similarity to angiomatoid variant of anaplastic carcinomas [2] . Aggressive nature of the tumor requires an early diagnosis and proper management of the case.
A case of angiosarcoma of the thyroid gland is being reported here for its rarity with a short review of literature.
2. Case History
A 60-year-old male presented to our department complaining of swelling in the neck for 20years with sudden increase in the size of the swelling and associated pain during last 3 months (Figure 1). There was no past history suggestive of any chronic medical or surgical illness. On clinical examination, the swelling was present in thyroid region, 10 × 8 cm size, firm, tender, mobile and moving with deglutition with normal skin mobility. No regional neck nodes were palpable. Rest of the ENT examination was unremarkable. Fine needle aspiration cytology revealed picture suggestive of anaplastic carcinoma. Thyroid status, chest X-ray and all other routine investigations were normal. CECT scan was done which showed 8.5 × 9.5 cm size mass with no lymphadenopathy. The patient underwent total thyroidectomy with central and lateral neck dissection under general anesthesia. During surgery, the capsule of the thyroid was found intact and there was no extension to the surrounding structures (Figure 2). The tissue was sent for histopathological examination. Post-operative period was uneventful.
On histopathology, grossly the external surface was congested. Cut surface showed large areas of necrosis in the centre with peripheral grey brown rim of tumor showing large areas of hemorrhage and few tiny colloid filled cysts. No capsular invasion was seen. Microscopic examination showed tumor tissue comprising predominantly of freely anastomosing vascular channels separated by large areas of fibrin and collagen deposition. At places vascular channels showed intraluminal growth forming papilla. These spaces were lined by atypical plump endothelial cells which were epitheloid in shape having high nucleocytoplasmic ratio, with vesicular nucleus having regular outline with predominantly basophilic nucleolus. At places nucleolus was connected to nuclear membrane by chromatin strand. Few bizarre cells and tumor giant cells were also seen. Mitotic count was 6 - 10 per high power field showing both atypical & typical cell forms. No evidence of capsular invasion was seen (Figure 3).

Figure 1. Patient showing the neck swelling.

Figure 2. Gross specimen of the tumor.
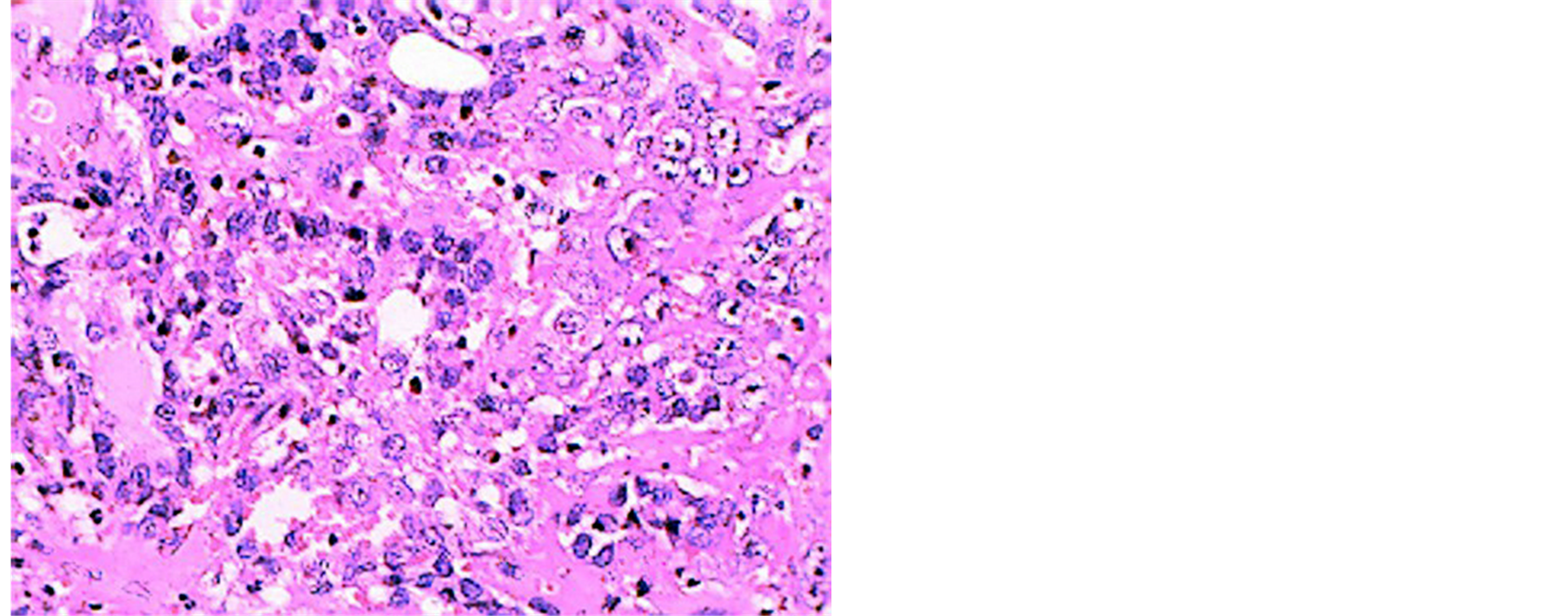
Figure 3. Histopathology slide of the tumor (Hematoxylin & Eosin stain, 100× magnification).
On histocytochemistry, masiontrichrome stain was positive for fibrin. Congo red with polorized microscopy was negative for amyloid. Immunohistochemistry for thyroglobulin was negative. It was positive for factor VIII, cluster of differentiation (CD31 and CD34) and negative for calcitonin, chromogranin, carcinoembryonic antigen (CEA) and epithelial membrane antigen (EMA).
Patient has received two cycles of chemotherapy consisting of cyclophosphamide and doxorubicin and 5-fluorouracil and has undergone radiotherapy (66 Gray) after chemotherapy. He is under follow up since last 10 months, with no recurrence of the tumor.
3. Discussion
Vascular tumors of the thyroid gland range from benign hemangiomas, such as infantile hemangioendothelioma, which regresses spontaneously to angiosarcoma which is locally very aggressive and carries a poor prognosis [7] . Originally, angiosarcoma used to be confined to only alpine regions. Now these tumors are also reported sporadically from non-mountainous areas like Hong Kong, northern France and coastal areas of US [8] . Here, we are reporting a case from India.
Angiosarcomas generally affect elderly females and have a long standing history of goiter with a recent rapid increase in size. Cases of long-standing nodular goiter are a real challenge for both the pathologist and the clinician/radiologist. Such lesions harbor a variety of pathologies. On fine needle aspiration cytology (FNAC), angiosarcoma closely mimics a number of different lesions, causing an erroneous diagnosis [3] . Therefore, the final diagnosis in such cases is generally made only after histopathology and immunohistochemistry analysis of the excised tumor. Immunopositivity for vascular markers for example, CD31, CD34, factor VIII related antigen, and absence of epithelial markers, greatly helps in diagnosis. But the distinction between angiosarcoma and anaplastic sarcomatoid carcinoma is difficult [2] [9] . Immunonegativity for thyroglobulin supports a diagnosis of angiosarcoma which is not found anaplastic carcinomas, confirming that these lesions are unrelated malignant tumors [10] . In our case also, the pathologist had a difficulty in diagnosing the tumor on cytopathology however the diagnosis was established with histopathology and immunohistochemistry.
Some authors doubt the existence of thyroid angiosarcoma, because they are of the opinion that the reported cases were being classified as anaplastic carcinomas with angiomatoid features. They are of the opinion that angiosarcomas are transitional tumors. These tumors show a variable appearance of mesenchymal metaplasia with both epithelial and endothelial differentiation. Angiosarcoma is the extreme in the spectrum of endothelial differentiation [2] [9] . WHO classification of thyroid tumors, published in 2004 has added the entity of poorly differentiated carcinoma and a variety of rare thyroid malignancies, such as angiosarcoma to its four traditional major tumor groups (papillary, follicular, medullary, and anaplastic carcinoma) [11] .
Besides the diagnosis, treating this tumor is also a challenge for a clinician due to its locally aggressive and destructive behaviour and a high recurrence rate. As regards adjuvant therapy, some say that, after the radical excision of the tumor, radiotherapy and then chemotherapy are indicated [6] ; others claim that, if the tumor is not corroded surgically and if the patient is subjected to radiotherapy and chemotherapy it represents only a palliative treatment because the first step of choice is radical surgical excision of the tumor. Regarding prognosis of the tumor, poor outcomes occur mostly with extracapsular tumor spread and distant metastasis [2] [4] [6] [8] . Data on survival are sparse. Goh et al. showed a 5-year survival rate of 33.3% [4] . But most of the patients die in less than 6 months regardless of the treatment with a few surviving up to 5 years [2] [8] . Entirely intrathyroid tumors generally have a longer survival than those with extrathyroidal extension [12] . Cases from non-mountainous, non-endemic goiter areas have a better prognosis [8] [12] .
In conclusion, though rare, angiosarcoma should be included as differential diagnosis in cases of long standing goiters with recent rapid increase in size. Histopathology and immunohistochemistry are very important tools for diagnosis and should be considered in such cases. As these tumors are very aggressive in nature, early and prompt diagnosis can help us in providing timely treatment in these patients.
References
- Sniezek, J.C. and Holten, M. (2003) Rare Tumors of the Thyroid Gland. Otolaryngologic Clinics of North America, 36, 107-115.
- Papotti, M., Arrondini, M., Tavaglione, V., Veltri, A. and Volante, M. (2008) Diagnostic Controversies in Vascular Proliferations of the Thyroid Gland. Endocrine Pathology, 19, 175-183. http://dx.doi.org/10.1007/s12022-008-9039-x
- Isa, N.M., James, D.T., Pennisi, R. and Gough, I. (2009) Primary Angiosarcoma of the Thyroid Gland with Recurrence Diagnosed by Fine Needle Aspiration: A Case Report. Diagnostic Cytopathology, 37, 427-432. http://dx.doi.org/10.1002/dc.21065
- Goh, S.G., Chuah, K.L., Goh, H.K. and Chen, Y.Y. (2003) Two Cases of Epithelioid Angiosarcoma Involving the Thyroid and a Brief Review of Non-Alpine Epithelioid Angiosarcoma of the Thyroid. Archives of Pathology & Laboratory Medicine, 127, 70-73.
- Petronella, P. (2012) Primary Thyroid Angiosarcoma: An Unusual Localization. World Journal of Surgical Oncology, 10, 73. http://dx.doi.org/10.1186/1477-7819-10-73
- Yilmazlar, T., Kirdak, T., Adim, S., Ozturk, E. and Yerci, O. (2005) A Case of Hemangiosarcoma in Thyroid with Severe Anemia Due to Bone Marrow Metastasis. Endocrine Journal, 52, 57-59. http://dx.doi.org/10.1507/endocrj.52.57
- Astl, J., Duskova, J., Limanova, Z., Povysil, C. and Kuchynkova, Z. (2000) Hemangiosarcoma of the Thyroid Gland. A Case Report. Neuro Endocrinology Letters, 21, 213-216.
- Hassan, I., et al. (2005) An Authentic Malignant Epithelioid Hemangioendothelioma of the Thyroid: A Case Report and Review of Literature. Thyroid, 12, 1377-1381. http://dx.doi.org/10.1089/thy.2005.15.1377
- Maiorana, A., Collina, G., Cesinaro, A.M., Fano, R.A. and Eusebi, V. (1996) Angiomatoid Carcinoma of the Thyroid: Clinicopathological Analysis of Seven Cases from Non-Alpine Areas. Virchows Arch, 429, 131-137.
- Ritter, J.H., Mills, S.E., Nappi, O. and Wick, M.R. (1995) Angiosarcoma-Like Neoplasms of Epithelial Organs: True Endothelial Tumors or Variants of Carcinoma? Seminars in Diagnostic Pathology, 12, 270-282.
- De Lellis, Ronald, A.D.L., Ricardo, V.L., Philipp, U.H. and Charis, E. (2004) Tumours of Endocrine Organs. In: WHO Classification of Tumours, WHO, Geneva, 113-114.
- Papotti, M., Volante, M., Negro, F., Eusebi, V. and Bussolati, G. (2000) Thyroglobulin mRNA Expression Helps to Distinguish Anaplastic Carcinoma from Angiosarcoma of the Thyroid. Virchows Arch, 437, 635-642. http://dx.doi.org/10.1007/s004280000308
NOTES

*Corresponding author.